Peer discussions and group study sessions centered around NCLEX Exam Questions can foster collaboration and enhance learning outcomes.
NCLEX Respiratory Health Problems Questions
Respiratory Health Problems NCLEX Practice Questions
Question 1.
A nurse is completing the health history for a client who has been taking Echinacea for a head cold. The client asks, “Why isn’t this helping me feel better?” Which response by the nurse would be the most accurate?
(a) “There is limited information as to the effec tiveness of herbal products.”
(b) “Antibiotics are the agents needed to treat a head cold.”
(c) "The head cold should be gone within the month.”
(d) “Combining herbal products with prescription antiviral medications is sure to help you.”
Answer:
(a) “There is limited information as to the effec tiveness of herbal products.”
Explanation:
At this time, there is no strong research evidence to warrant recommendations of herbal products for management of colds; further study is needed to show evidence of therapeutic effects and indications. Antibiotics are effective against bacteria; the head cold may have a viral cause. An uncomplicated upper respiratory tract infection subsides within 2 to 3 weeks. There may be a drug-drug interaction with herbal products and prescriptions.
Question 2.
A nurse is teaching a client about taking anti-histamines. Which information should the nurse include in the teaching plan? Select all that apply.
(a) Operating machinery and driving may be dangerous while taking antihistamines.
(b) Continue taking antihistamines even if nasal infection develops.
(c) The effect of antihistamines is not felt until a day later.
(d) Do not use alcohol with antihistamines.
(e) Increase fluid intake to 2,000 mL/day.
Answer:
(a) Operating machinery and driving may be dangerous while taking antihistamines.
(d) Do not use alcohol with antihistamines.
(e) Increase fluid intake to 2,000 mL/day.
Explanation:
(a), (d), (e). Antihistamines have an anticholinergic action and a drying effect and reduce nasal, salivary, and lacrimal gland hypersecretion (runny nose, tearing, and itching eyes). An adverse effect is drowsiness, so operating machinery and driving are not recommended. There is also an additive depressant effect when alcohol is combined with antihistamines, so alcohol should be avoided during antihistamine use. The client should ensure adequate fluid intake of at least 2,000 mL (about eight glasses) per day due to the drying effect of the drug. Antihistamines have no antibacterial action and are not used to treat nasal infections. The effect of antihistamines is prompt, not delayed.
Question 3.
A nurse instructs a client with allergic rhinitis about the correct technique for using an intranasal inhaler. Which statement indicates that the client understands the instructions?
(a) “I should limit the use of the inhaler to early morning and bedtime use.”
(b) “It is important to not shake the canister because that can damage the spray device.”
(c) “I should hold one nostril closed while I insert the spray into the other nostril.”
(d) "The inhaler tip is inserted into the nostril and pointed toward the inside nostril wall.”
Answer:
(c) “I should hold one nostril closed while I insert the spray into the other nostril.”
Explanation:
When using an intranasal inhaler, it is important to close off one nostril while inhaling the spray into the other nostril to ensure the best inhalation of the spray. Use of the inhaler is not limited to mornings and bedtime. The canister should be shaken immediately before use. The inhaler tip should be inserted into the nostril and pointed toward the outside nostril wall to maximize inhalation of the medication.
Question 4.
The nurse is evaluating the effectiveness of a teaching plan for a client recovering from an upper respiratory tract infection. Which is an expected outcome of the plan? The client will:
(a) maintain a fluid intake of 800 mL every 24 hours.
(b) have a temperature below 100°F (37.8°C).
(c) cough productively without chest discomfort.
(d) experience less nasal obstruction and discharge.
Answer:
(d) experience less nasal obstruction and discharge.
Explanation:
A client recovering from an upper respiratory tract infection should report decreasing or no nasal discharge and obstruction. Daily fluid intake should be increased to more than 1 L every 24 hours to liquefy secretions. The temperature should be below 100°F (37.8°C) with no chills or diaphoresis. A productive cough with chest pain indicates a pulmonary infection, not an upper respiratory tract infection.
Question 5.
The nurse teaches the client how to instill nose drops. Which technique is correct?
(a) The client uses sterile technique when handling the dropper.
(b) The client blows the nose gently before instilling drops.
(c) The client uses a new dropper for each instillation.
(d) The client sits in a semi-Fowler’s position for 2 minutes.
Answer:
(b) The client blows the nose gently before instilling drops.
Explanation:
The client should blow the nose before instilling nose drops. Instilling nose drops is a clean technique. The dropper should be cleaned after each administration, but it does not need to be changed. The client should assume a position that will allow the medication to reach the desired area; this is usually a supine position.
Question 6.
The nurse should include which instructions in the teaching plan for a client with chronic sinusitis? Select all that apply.
(a) Avoid the use of caffeinated beverages.
(b) Perform postural drainage every day.
(c) Take a hot shower in the morning and evening.
(d) Report a temperature of 102°F (38.9°C) or higher.
(e) Limit fluid intake to 1,000 mL per 24 hours.
Answer:
(c) Take a hot shower in the morning and evening.
(d) Report a temperature of 102°F (38.9°C) or higher.
Explanation:
(c), (d). The client with chronic sinusitis should be instructed to take hot showers in the morning and evening to promote drainage of secretions. There is no need to limit caffeine intake. Performing postural drainage will inhibit removal of secretions, not promote it. Clients should elevate the head of the bed to promote drainage. Clients should report all temperatures higher than 100.4°F (38°C) because a temperature that high can indicate infection. The client should increase, not limit, fluid intake; a 24-hour fluid intake of 2,000 to 3,000 mL would be appropriate.
Question 7.
A client with allergic rhinitis asks the nurse what to do to decrease rhinorrhea. Which instruction would be appropriate for the nurse to give the client?
(a) “Use your nasal decongestant spray regularly to help clear your nasal passages.”
(b) “Ask the health care provider for antibiotics. Antibiotics will help decrease the secretion.”
(c) “It is important to increase your activity. A daily brisk walk will help promote drainage.”
(d) “Keep a diary of when your symptoms occur. This can help you identify what precipitates your attacks.”
Answer:
(d) “Keep a diary of when your symptoms occur. This can help you identify what precipitates your attacks.”
Explanation:
It is important for clients with allergic rhinitis to determine the precipitating factors so that they can be avoided. Keeping a diary can help identify these triggers. Nasal decongestant sprays should not be used regularly because they can cause a rebound effect. Antibiotics are not appropriate for allergic rhinitis because an infection is not present. Increasing activity will not control the client’s symptoms; in fact, walking outdoors may increase them if the client is allergic to pollen.
Question 8.
The health care provider (HCP) has prescribed guaifenesin 300 mg four times a day. The dosage strength of the liquid is 200 mg/5 mL. How many milliliters should the nurse administer for each dose? Record your answer using one decimal place.
..................... mL.
Answer:
7.5 mL
300 mg/x = 200 mg/5 mL
x = 7.5 mL.
Question 9.
The health care provider (HCP) has prescribed pseudoephedrine. The nurse should instruct the client about which possible adverse effects of this drug.
(a) constipation
(b) bradycardia
(c) diplopia
(d) restlessness
Answer:
(d) restlessness
Explanation:
Adverse effects of pseudoephedrine are experienced primarily in the cardiovascular system and through sympathetic effects on the central nervous system (CNS). The most common CNS adverse effects include restlessness, dizziness, tension, anxiety, insomnia, and weakness. Common cardiovascular adverse effects include tachycardia, hypertension, palpitations, and arrhythmias. Constipation and diplopia are not adverse effects of pseudoephedrine. Tachycardia, not bradycardia, is an adverse effect of pseudoephedrine.
Question 10.
A healthcare provider (HCP) has just inserted nasal packing for a client with epistaxis. The client is taking ramipril for hypertension. What should the nurse instruct the client to do?
(a) Use 81 mg of aspirin daily for relief of discomfort.
(b) Omit the next dose of ramipril.
(c) Remove the packing if there is difficulty swallowing.
(d) Avoid rigorous aerobic exercise.
Answer:
(d) Avoid rigorous aerobic exercise.
Explanation:
Epistaxis, or nosebleeds, is a common, sudden emergency. Commonly, no apparent explanation for the bleeding is known. With significant blood loss, systemic symptoms, such as vertigo, increased pulse, shortness of breath, decreased blood pressure, and pallor will occur. Because aerobic exercise may increase blood pressure and increased blood pressure can cause epistaxis, the client with hypertension should avoid it. Aspirin inhibits platelet aggregation, reducing the ability of the blood to clot. The client should continue to take his antihypertension medication, ramipril. Posterior nasal packing should be left in place for 1 to 3 days.
Question 11.
A client had surgery for a deviated nasal septum. Which finding indicates that bleeding is occurring even if the nasal drip pad remains dry and intact?
(a) nausea
(b) repeated swallowing
(c) increased respiratory rate
(d) increased pain
Answer:
(b) repeated swallowing
Explanation:
Because of the dense nasal packing, bleeding may not be apparent through the nasal drip pad. Instead, the blood may run down the throat, causing the client to swallow frequently. The back of the throat, where the blood will be apparent, can be assessed with a flashlight. An accumulation of blood in the stomach can cause nausea and vomiting, but nausea would not be the initial indicator of bleeding. An increased respiratory rate occurs in shock but is not an early sign of bleeding in a client who has undergone nasal surgery. Increased pain warrants further assessment but is not an indicator of bleeding.
Question 12.
A client who has undergone outpatient nasal surgery is ready for discharge and has nasal packing in place. What should the nurse instruct the client to do?
(a) Avoid activities that elicit Valsalva’s maneuver.
(b) Take aspirin to control nasal discomfort.
(c) Avoid brushing the teeth until the nasal packing is removed.
(d) Apply heat to the nasal area to control swelling.
Answer:
(a) Avoid activities that elicit Valsalva’s maneuver.
Explanation:
The client should be instructed to avoid any activities that cause Valsalva’s maneuver (e.g., constipation, vigorous coughing, exercise) in order to reduce bleeding and stress on suture lines. The client should not take aspirin because of its antiplatelet properties, which may cause bleeding. Oral hygiene is important to rid the mouth of old dried blood and to enhance the client’s appetite. Cool compresses, not heat, should be applied to decrease swelling and control discoloration of the area.
Question 13.
Which statement indicates to the nurse that a client has understood the discharge instructions provided after nasal surgery?
(a) “I should not shower until my packing is removed.”
(b) “I will take stool softeners and modify my diet to prevent constipation.”
(c) “Coughing every 2 hours is important to prevent respiratory complications.”
(d) “It is important to blow my nose each day to remove the dried secretions.”
Answer:
(b) “I will take stool softeners and modify my diet to prevent constipation.”
Explanation:
Constipation can cause straining during defecation, which can induce bleeding. Showering is not contraindicated. The client should take measures to prevent coughing, which can cause bleeding. The client should avoid blowing the nose for 48 hours after the packing is removed. Thereafter, the client should blow the nose gently, using the open-mouth technique to minimize bleeding in the surgical area.
Question 14.
The nurse is giving preoperative instructions to a client who will be undergoing rhinoplasty. What should the nurse tell the client?
(a) “After surgery, nasal packing will be in place for 7 to 10 days.”
(b) “Normal saline nose drops will need to be administered preoperatively.”
(c) “The results of the surgery will be immediately obvious postoperatively.”
(d) “Do not take aspirin-containing medications for 2 weeks before surgery.”
Answer:
(d) “Do not take aspirin-containing medications for 2 weeks before surgery.”
Explanation:
Aspirin-containing medications should be discontinued for 2 weeks before surgery to decrease the risk of bleeding. Nasal packing is usually removed the day after surgery. Normal saline nose drops are not routinely administered preopera- tively. The results of the surgery will not be obvious immediately after surgery because of edema and ecchymosis.
Question 15.
A client has had surgery for a deviated nasal septum. The client has returned from the postanesthesia care unit. What should the nurse do first?
(a) Assess the client’s pain.
(b) Inspect the area for periorbital ecchymosis.
(c) Assess respiratory status.
(d) Measure intake and output.
Answer:
(c) Assess respiratory status.
Explanation:
Immediately after nasal surgery, ineffective breathing patterns may develop as a result of the nasal packing and nasal edema. Nasal packing may dislodge, leading to obstruction. Assessing for airway obstruction is a priority. Assessing for pain is important, but it is not as high a priority as assessment of the airways. It is too early to detect ecchymosis. Measuring intake and output is not typically a priority £TJ nursing assessment after nasal surgery.
Question 16.
After nasal surgery, the client expresses concern about how to decrease facial pain and swelling while recovering at home. Which instruction would be most effective for decreasing pain and edema?
(a) Take analgesics every 4 hours around the clock.
(b) Use corticosteroid nasal spray as needed to control symptoms.
(c) Use a bedside humidifier while sleeping.
(d) Apply cold compresses to the area.
Answer:
(d) Apply cold compresses to the area.
Explanation:
Applying cold compresses helps to decrease facial swelling and pain from edema. Analgesics may decrease pain, but they do not decrease edema. A corticosteroid nasal spray would not be administered postoperatively because it can impair healing. Use of a bedside humidifier promotes comfort by providing moisture for nasal mucosa, but it does not decrease edema.
Question 17.
A client is being discharged with nasal packing in place. What should the nurse instruct the client to do?
(a) Perform frequent mouth care.
(b) Use normal saline nose drops daily.
(c) Sneeze and cough with mouth closed.
(d) Gargle every 4 hours with salt water.
Answer:
(a) Perform frequent mouth care.
Explanation:
Frequent mouth care is important to provide comfort and encourage eating. Mouth care promotes moist mucous membranes. Nose drops cannot be used with nasal packing in place. When sneezing and coughing, the client should do so with the mouth open to decrease the chance of dislodging the packing. Gargling should not be attempted with packing in place.
Question 18.
The nurse is teaching a client how to manage a nosebleed. What instruction should the nurse give the client?
(a) “Tilt your head backward, and pinch your nose.”
(b) “Lie down flat, and place an ice compress over the bridge of the nose.”
(c) “Blow your nose gently with your neck flexed.”
(d) “Sit down, lean forward, and pinch the soft portion of your nose.”
Answer:
(d) “Sit down, lean forward, and pinch the soft portion of your nose.”
Explanation:
The client should assume a sitting position and lean forward. Firm pressure should be applied to the soft portion of the nose for approximately 10 minutes. Tilting the head backward can cause the client to swallow blood, which can obscure the amount of bleeding and also can lead to nausea. Ice compresses may be applied, but the client should not lie flat. Blowing the nose is to be avoided because it can increase bleeding.
Question 19.
A client had posterior packing inserted to control a severe nosebleed. After insertion of the packing, the nurse should observe the client for which finding?
(a) vertigo
(b) Bell’s palsy
(c) hypoventilation
(d) loss of gag reflex
Answer:
(c) hypoventilation
Explanation:
Posterior packing may alter the respiratory status of the client, especially in older adults clients, causing hypoventilation. Clients should be observed carefully for changes in level of consciousness, respiratory rate, and heart rate and rhythm after the insertion of the packing. Vertigo does not occur as a result of the insertion of posterior packing. Bell’s palsy, a disorder of the seventh cranial nerve, is not associated with epistaxis or nasal pack-ing. Loss of gag reflex does not occur as a result of the insertion of posterior packing.
Question 20.
A client has had a radical neck dissection for laryngeal cancer. Which action is the priority for nursing care immediately following this surgery?
(a) maintaining complete bed rest until postsur- gical swelling decreases
(b) taking vital signs once a shift until the client is stable
(c) determining if the client can swallow
(d) suctioning the laryngectomy tube as often as needed
Answer:
(d) suctioning the laryngectomy tube as often as needed
Explanation:
The nurse must maintain patency of the airway with frequent suctioning of the laryngectomy
tube that can become occluded from secretions, blood, and mucus plugs. Once the client is hemo- dynamically stable, getting out of bed should be encouraged to prevent postoperative complications. Vital signs should be monitored more frequently in a postoperative client. A swallow study is done at approximately 5 to 7 days after surgery, prior to starting oral intake.
Question 21.
A client who has had a total laryngectomy appears withdrawn and depressed. The client keeps the curtain drawn, refuses visitors, and indicates a desire to be left alone. Which nursing intervention would be most therapeutic for the client?
(a) discussing the behavior with the spouse to determine the cause
(b) exploring future plans
(c) respecting the need for privacy
(d) encouraging expression of feelings nonverbally and in writing
Answer:
(d) encouraging expression of feelings nonverbally and in writing
Explanation:
The client has undergone body changes and permanent loss of verbal communication. He may feel isolated and insecure. The nurse can encourage him to express his feelings and use this information to develop an appropriate plan of care. Discussing the client’s behavior with his wife may not reveal his feelings. Exploring future plans is not appropriate at this time because more information about the client’s behavior is needed before proceeding to this level. The nurse can respect the client’s need for privacy while also encouraging him to express his feelings.
Question 22.
The nurse is suctioning a client who had a laryngectomy. What is the maximum amount of time the nurse should suction the client?
(a) 10 seconds
(b) 20 seconds
(c) 25 seconds
(d) 30 seconds
Answer:
(a) 10 seconds
Explanation:
A client should be suctioned for no longer than 10 seconds at a time. Suctioning for longer than 10 seconds may reduce the client’s oxygen level so much that the client becomes hypoxic.
Question 23.
What should the nurse do when suctioning a client who has a tracheostomy tube 3 days following insertion?
(a) Use a sterile catheter each time the client is suctioned.
(b) Clean the catheter in sterile water after each use, and reuse for no longer than 8 hours.
(c) Protect the catheter in sterile packaging between suctioning episodes.
(d) Use a clean catheter with each suctioning, and disinfect it in hydrogen peroxide between uses.
Answer:
(a) Use a sterile catheter each time the client is suctioned.
Explanation:
The recommended technique is to use a sterile catheter each time the client is suctioned. There is a danger of introducing organisms into the respiratory tract when strict aseptic technique is not used. Reusing a suction catheter is not consistent with aseptic technique. The nurse does not use a clean catheter when suctioning a tracheostomy or a laryngectomy; it is a sterile procedure.
Question 24.
The client with a laryngectomy does not want to be observed by the family because the opening in the throat is “disgusting.” How should the nurse respond to the client?
(a) Initiate teaching about the care of a stoma.
(b) Explain that the stoma will not always look as it does now.
(c) Inform the client of the benefits of family support at this time.
(d) Explore why the client believes the stoma is “disgusting.”
Answer:
(d) Explore why the client believes the stoma is “disgusting.”
Explanation:
Changes in body image are expected after a laryngectomy, and the nurse should first explore what is upsetting the client the most at this time. Many clients are concerned about how their family members will respond to the physical changes that have occurred as a result of a laryngectomy, but discussing the importance of family support is not helpful; instead, the nurse should allow the client to communicate any negative feelings or concerns that exist because of the surgery. The client’s feelings are not related to a knowledge deficit, and therefore, it is too early to begin teaching about stoma care. It is also not helpful to offer reassurances about the change in appearance; the client will require time to adjust to the changed body image.
Question 25.
The nurse team leader is making rounds and observes the client who had a tracheostomy tube inserted 2 days ago (see figure). The nursing policy manual recommends the use of the gauze pad. What should the nurse do?
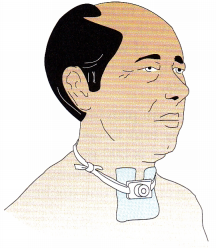
(a) Make sure the gauze pad is dry and the client is in a comfortable position.
(b) Ask the unlicensed assistive personnel to tie the tracheostomy tube ties in the back of the client’s neck.
(c) Reposition the gauze pad around the stoma with the open end downward.
(d) Ask a registered nurse to change the ties and position another gauze pad around the stoma.
Answer:
(a) Make sure the gauze pad is dry and the client is in a comfortable position.
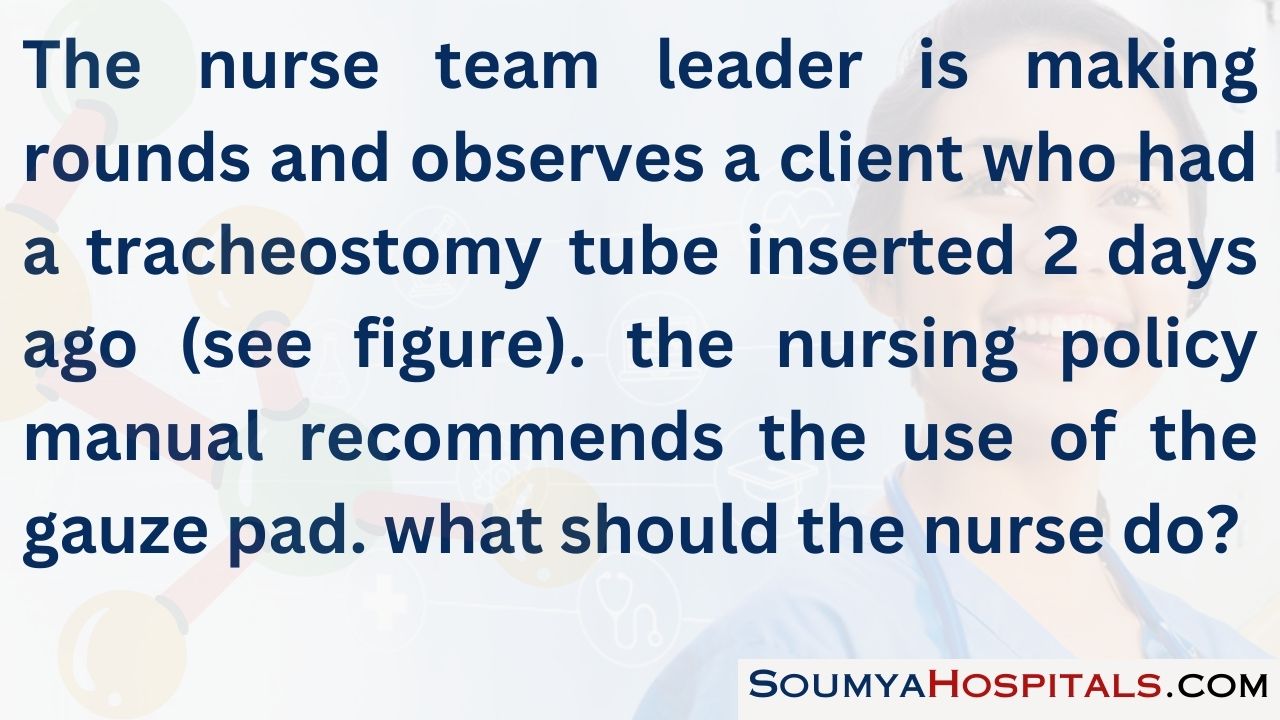
Explanation:
The tracheostomy tube, ties, and gauze pad are positioned correctly; the nurse team leader should be sure the client is comfortable. The tracheostomy tube ties should be tied in a square knot on the side of the neck and alternate sides of the neck when the ties are changed. The full part of the gauze square should be placed under the tracheostomy tube to absorb drainage. There is no indication the ties need to be changed; an additional gauze pad is not necessary; if necessary, the current gauze square should be changed rather than adding an additional pad.
Question 26.
To reduce the risk of laryngeal cancer in employees in a factory that uses respiratory irritants, what instructions should the nurse give the employees? Select all that apply.
(a) Stop smoking.
(b) Use a portable high-efficiency particulate air(HEPA) air purifier in the home.
(c) Limit alcohol intake.
(d) Brush teeth after every meal.
(e) Avoid raising the voice to be heard over the noise in the factory.
Answer:
(a) Stop smoking.
(c) Limit alcohol intake.
Explanation:
(a), (c). The primary risk factors for laryngeal cancer are smoking and alcohol abuse. Smoking cessation is most successful with a support group or counseling. Heavy drinking should be avoided since the risk increases with amount of alcohol consumption. HEPA filters help trap small particles and allergens to reduce allergy symptoms and asthma. Poor oral hygiene is not a risk factor, nor is overusing the voice.
Question 27.
A client has had hoarseness for more than 2 weeks. What should the nurse do?
(a) Refer the client to a health care provider for a prescription for an antibiotic.
(b) Instruct the client to gargle with salt water at home.
(c) Assess the client for dysphagia.
(d) Instruct the client to take a throat analgesic.
Answer:
(c) Assess the client for dysphagia.
Explanation:
Hoarseness occurring longer than 2 weeks is a warning sign of laryngeal cancer. The nurse should first assess other signs, such as a lump in the neck or throat, persistent sore throat or cough, earache, pain, and difficulty swallowing (dysphagia). Gargling with salt water may lead to increased irritation. There is no indication of infection warranting an antibiotic. An oral analgesic would provide only temporary relief of discomfort if hoarseness is accompanied by a sore throat.
Question 28.
A client has just returned from the postanesthesia care unit after undergoing a laryngectomy. Which instruction should the nurse include in the plan of care?
(a) Maintain the head of the bed at 30 to 40 degrees.
(b) Teach the client how to use esophageal speech.
(c) Initiate small feedings of soft foods.
(d) Irrigate drainage tubes as needed.
Answer:
(a) Maintain the head of the bed at 30 to 40 degrees.
Explanation:
Immediately after surgery, the client should be maintained in a position with the head of the bed elevated 30 to 40 degrees (semi-Fowler’s position) to decrease tissue edema, facilitate breathing, and decrease pain related to edema formation. Immediately postoperatively, the client should be provided alternative means of communicating, such as a communication board. As healing progresses and edema subsides, a speech therapist should work with the client to explore various voice restoration options, such as the use of a voice prosthesis, electrolarynx, artificial larynx, or esophageal speech. Food is not initiated in the immediate postoperative phase; enteral feedings are usually used to meet nutritional needs until edema subsides. Irrigation of the drainage tubes is an inappropriate action.
Question 29.
The nurse is making a discharge plan for a client recovering from a total laryngectomy. What is an expected outcome?
The client will:
(a) regain the ability to taste and smell food.
(b) demonstrate appropriate care of the gastrostomy tube.
(c) communicate feelings about body image changes.
(d) demonstrate sterile suctioning technique for stoma care.
Answer:
(c) communicate feelings about body image changes.
Explanation:
It is important that the client be able to communicate his or her feelings about the body image changes that have occurred as a result of surgery. Open communication helps promote adjustment. The client may not regain the ability to taste and smell food because of no longer breathing through the nose or because of radiation therapy treatments, or both. A gastrostomy tube would not typically be placed after a total laryngectomy, nor would it be necessary for the client to demonstrate sterile suctioning technique for stoma care. The client would use clean technique.
Question 30.
What instruction should the nurse give the client who underwent a laryngectomy and is now going home?
(a) Perform mouth care every morning and evening.
(b) Provide adequate humidity in the home.
(c) Maintain a soft, bland diet.
(d) Limit physical activity to shoulder and neck exercises.
Answer:
(b) Provide adequate humidity in the home.
Explanation:
Adequate humidity should be provided in the home to help keep secretions moist. A bedside humidifier is recommended. A high fluid intake is also important to liquefy secretions. Mouth care is important to prevent drying of mucous membranes and should be performed frequently throughout the day, especially before and after meals, to help stimulate appetite. The client may eat any food that can be chewed and swallowed comfortably. The client may resume physical activity as tolerated.
Question 31.
The nurse is caring for a client with bacterial pneumonia. The effectiveness of the client’s oxygen therapy can be best determined by which indicator of oxygenation?
(a) absence of cyanosis
(b) client’s respiratory rate
(c) arterial blood gas (ABG) values
(d) client’s level of consciousness
Answer:
(c) arterial blood gas (ABG) values
Explanation:
The client’s ABC levels are the most sensitive indicator of the effectiveness of the client’s oxygen therapy. Cyanosis is a late sign of decreased oxygenation and is not a reliable indicator. The client’s respiratory rate and level of consciousness may be altered because of other problems not related to the client’s oxygenation.
Question 32.
A client admitted with pneumonia and dementia has attempted several times to pull out the IV and Foley catheter. After trying other options, the nurse obtains a prescription for bilateral soft wrist restraints. Which nursing action is most appropriate?
(a) Perform circulation checks to bilateral upper extremities each shift.
(b) Attach the ties of the restraints to the bed frame.
(c) Reevaluate the need for restraints and document weekly.
(d) Ensure the restraint prescription has been signed by the health care provider (HCP) within 72 hours.
Answer:
(b) Attach the ties of the restraints to the bed frame.
Explanation:
Restraints should be secured to the bed frame, not the side rails, to ensure that the side rails can be raised and lowered safely. Circulation checks, reevaluating need for restraints, and documentation should be done every 1 to 2 hours. Medical restraint prescriptions must be renewed and signed by an HCP every 24 hours.
Question 33.
A client is admitted to the hospital with a diagnosis of bacterial pneumonia. While obtaining the client’s health history, the nurse learns that the client has osteoarthritis, follows a vegetarian diet, and is very concerned with cleanliness. Which client information would most likely be a predisposing factor for the diagnosis of pneumonia?
(a) age
(b) osteoarthritis
(c) vegetarian diet
(d) daily bathing
Answer:
(a) age
Explanation:
The client’s age is a predisposing factor for pneumonia; pneumonia is more common in older or debilitated clients. Other predisposing factors include smoking, upper respiratory tract infections, malnutrition, immunosuppression, and the presence of a chronic illness. Osteoarthritis, a nutritionally sound vegetarian diet, and frequent bathing are not predisposing factors for pneumonia.
Question 34.
A client with bacterial pneumonia is to be started on IV antibiotics. The nurse should verify that which diagnostic test has been completed before administering the antibiotic?
(a) urinalysis
(b) sputum culture
(c) chest radiograph
(d) red blood cell count
Answer:
(b) sputum culture
Explanation:
A sputum specimen is obtained for culture to determine the causative organism. After the organism is identified, an appropriate antibiotic can be prescribed. Beginning antibiotic therapy before obtaining the sputum specimen may alter the results of the test. Urinalysis, a chest radiograph, and a red blood cell count do not need to be obtained before initiation of antibiotic therapy for pneumonia.
Question 35.
When caring for the client who is receiving an aminoglycoside antibiotic, the nurse should monitor which laboratory value?
(a) serum sodium
(b) serum potassium
(c) serum creatinine
(d) serum calcium
Answer:
(c) serum creatinine
Explanation:
It is essential to monitor serum creatinine in the client receiving an aminoglycoside antibiotic because of the potential of this type of drug to cause acute tubular necrosis. Aminoglycoside antibiotics do not affect serum sodium, potassium, or calcium levels.
Question 36.
A client with pneumonia has a temperature of 102.6°F (39.2°C), is diaphoretic, and has a productive cough. The client is able to ambulate. What should the nurse do?
(a) Change the client’s position every 4 hours.
(b) Use nasotracheal suctioning to clear secretions.
(c) Change the bedsheets frequently.
(d) Offer the use of a bedpan every 2 hours.
Answer:
(c) Change the bedsheets frequently.
Explanation:
Frequent changes of the bedsheets are appropriate for this client because of the diaphoresis. Diaphoresis produces general discomfort, and the client should be kept dry to promote comfort and prevent skin irritation. The client should change position every 2 hours. Nasotracheal suc-tioning is not indicated with the client’s productive cough. The client can ambulate to the bathroom, but the nurse should offer assistance as needed.
Question 37.
Which nursing action would most likely be successful in reducing pleuritic chest pain in a client with pneumonia?
(a) Encourage the client to breathe shallowly.
(b) Have the client practice abdominal breathing.
(c) Offer the client incentive spirometry.
(d) Teach the client to splint the rib cage when coughing.
Answer:
(d) Teach the client to splint the rib cage when coughing.
Explanation:
The pleuritic pain is triggered by chest movement and is particularly severe during coughing. Splinting the chest wall will help reduce the discomfort of coughing. Deep breathing is essential to prevent further atelectasis. Abdominal breathing is not as effective in decreasing pleuritic chest pain as is splinting of the rib cage. Incentive spirometry facilitates effective deep breathing but does not decrease pleuritic chest pain.
Question 38.
The nurse administers two 325-mg aspirin every 4 hours to a client with pneumonia. The nurse should evaluate the outcome of administering the drug by assessing the client for which findings? Select all that apply.
(a) decreased pain when breathing
(b) prolonged clotting time
(c) decreased temperature
(d) decreased respiratory rate
(e) increased ability to expectorate secretions
Answer:
(a) decreased pain when breathing
(c) decreased temperature
Explanation:
Aspirin is administered to clients with pneumonia because it is an analgesic that helps control chest discomfort and an antipyretic that helps reduce fever. Aspirin has an anticoagulant effect, but that is not the reason for prescribing it for a client with pneumonia, and the use of the drug will be short term. Aspirin does not affect the respiratory rate and does not facilitate expectoration of secretions.
Question 39.
Which mental status change may occur when a client with pneumonia is first experiencing hypoxia?
(a) coma
(b) apathy
(c) irritability
(d) depression
Answer:
(c) irritability
Explanation:
Clients who are experiencing hypoxia characteristically exhibit irritability, restlessness, or anxiety as initial mental status changes. As the hypoxia becomes more pronounced, the client may become confused and combative. Coma is a late clinical manifestation of hypoxia. Apathy and depression are not symptoms of hypoxia.
Question 40.
Which is an expected finding for a client who has been treated for bacterial pneumonia?
(a) a respiratory rate of 25 to 30 breaths/min
(b) the ability to perform activities of daily living without dyspnea
(c) a maximum loss of 5 to 10 lb (2 to 5 kg) of body weight
(d) chest pain that is minimized by splinting the rib cage
Answer:
(b) the ability to perform activities of daily living without dyspnea
Explanation:
An expected outcome for a client recovering from pneumonia would be the ability to perform activities of daily living without experiencing dyspnea. A respiratory rate of 25 to 30 breaths/min indicates the client is experiencing tachypnea, which would not be expected on recovery. A weight loss of 5 to 10 lb (2.27 to 4.53 kg) is undesirable; the expected outcome would be to maintain normal weight. A client who is recovering from pneumonia should experience decreased or no chest pain.
Question 41.
A client newly diagnosed with tuberculosis (TB) is being admitted with the prescription for “isolation precautions for tuberculosis.” The nurse should assign the client to which type of room?
(a) a room at the end of the hall for privacy
(b) a private room to implement airborne precautions
(c) a room near the nurses’ station to ensure confidentiality
(d) a room with windows to allow sunlight
Answer:
(a) a room at the end of the hall for privacy
Explanation:
Implementing airborne precautions for possible TB requires a private room assignment. In addition to isolating the client by using a private room, engineering controls can help prevent the spread of TB; a room at the end of the hall will aid in controlling airflow direction and can prevent con-tamination of air in adjacent areas. Confidentiality is provided for every client, regardless of the client’s room location. Sunlight is not a component of isolation precautions.
Question 42.
The nurse is reviewing the history and physical and health care provider prescriptions on the medical record of a newly admitted client.
|
Subjective: |
19-year-old reports a constant cough for the past "few weeks" with "dark" sputum for the past few days. Has night sweats, 10-lb (4.5-kg) weight loss in the past month, and "always" being tired. He took one Tylenol about an hour prior to arrival. |
|
Objective: |
|
|
BP |
120/64 |
|
HR |
84/reg |
|
Resp |
26/unlabored/slight wheezing in right lower lobe posteriorly |
|
02 Sat |
92% |
|
Temp |
99.9°F (37.7°C) oral |
|
Skin |
Warm, slightly diaphoretic |
|
Nonproductive cough at this time |
|
|
Assessment: |
Possible respiratory infection |
|
Physician prescriptions tab |
|
|
|
Chest X-ray |
|
|
Sputum specimen |
|
|
Oxygen at 2 L per nasal cannula |
What should the nurse do first?
(a) Initiate airborne precautions.
(b) Apply oxygen at 2 L per nasal cannula.
(c) Collect a sputum sample.
(d) Reassess vital signs.
Answer:
(a) Initiate airborne precautions.
Explanation:
There is a high risk and potential for tuberculosis, and airborne precautions should be implemented immediately to prevent the spread of infection. After initiating precautions, the nurse can start the oxygen, check the vital signs, and collect the sputum specimen.
Question 43.
A client is receiving streptomycin to treat tuberculosis. What should the nurse evaluate to determine an adverse effect of the drug?
(a) decreased serum creatinine
(b) difficulty swallowing
(c) hearing loss
(d) IV infiltration
Answer:
(c) hearing loss
Explanation:
Streptomycin can cause toxicity to the eighth cranial nerve, which is responsible for hearing, balance, and body position sense. Nephrotoxicity is a side effect that would be indi-cated with an increase in creatinine. Streptomycin does not cause difficulty in swallowing. Streptomycin is given via intramuscular injection.
Question 44.
The nurse is reconciling the prescriptions for a client diagnosed recently with pulmonary tuberculosis who is being admitted to the hospital for a total hip replacement (see medication prescription sheet). The client asks if it is necessary to take all of these medications while in the hospital. What should the nurse tell the client?
Medication Prescription
- isoniazid (INH), 300 mg PO daily
- Rifampin (Rifadin), 600 mg PO daily
- Pyridoxine (vitamin B6), 10 mg PO daily
- ethambutol, 400 mg PO daily
- pyrazinamide, 1.5 g PO daily
(a) I’ll ask your health care provider (HCP) to review the prescriptions for duplication between isoniazid and ethambutol.”
(b) “I can’t discontinue any of these drugs until you can eat solid foods.”
(c) “I’ll ask the pharmacist to check for drug interactions between the rifampin and isoniazid.”
(d) It’s important to continue to take the medications because the combination of drugs prevents bacterial resistance.”
Answer:
(d) It’s important to continue to take the medications because the combination of drugs prevents bacterial resistance.”
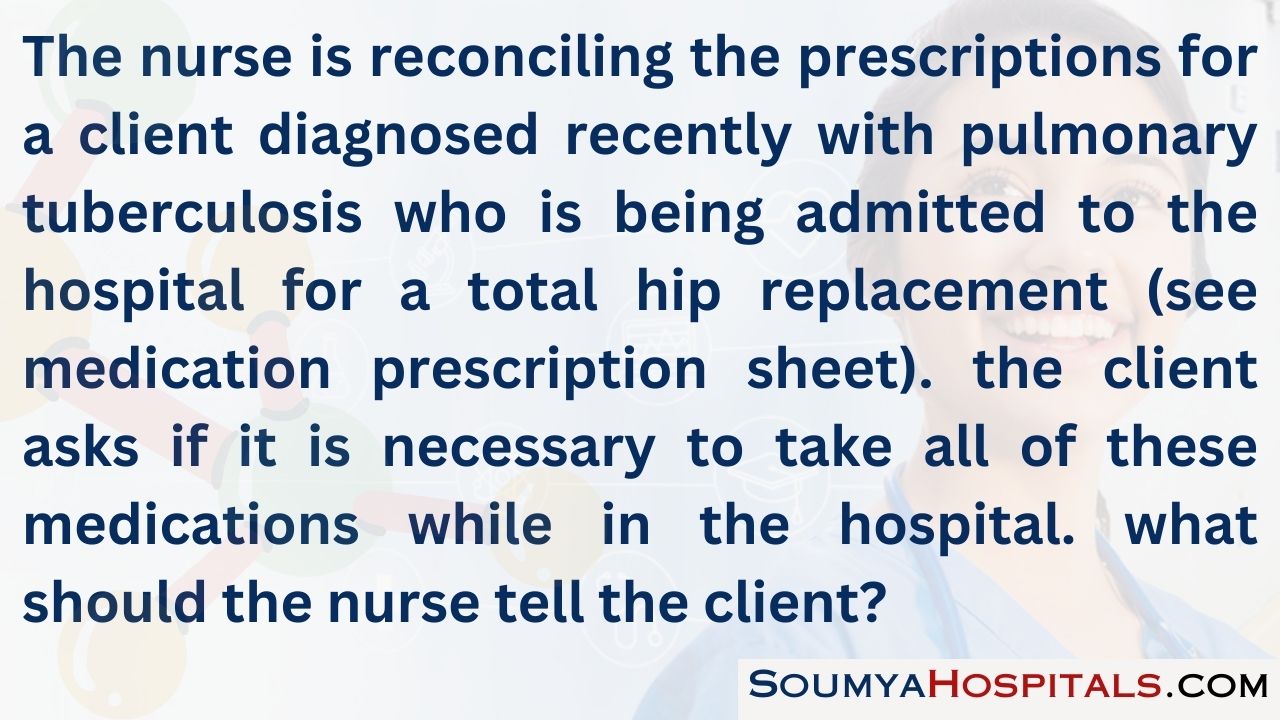
Explanation:
The nurse should tell the client that it is necessary to take all of these medications because combination drug therapy prevents bacterial resistance; they will be administered throughout the hospitalization to maintain blood levels. The HCP CO will review the prescriptions per hospital policy because the client is being admitted to the hospital; there is no duplication between any of the drugs being prescribed for this client. It is not necessary to ask the pharmacist to check for drug interactions as these drugs are commonly used together.
Question 45.
The client with tuberculosis is to be discharged home with nursing follow-up. Which aspect of nursing care will have the highest priority?
(a) offering the client emotional support
(b) teaching the client about the disease and its treatment
(c) coordinating various agency services
(d) assessing the client’s environment for sanitation
Answer:
(b) teaching the client about the disease and its treatment
Explanation:
Ensuring that the client is well-educated about tuberculosis is the highest priority. Education of the client and family is essential to help the client understand the need for completing the prescribed drug therapy to cure the disease. Offering the client emotional support, coordinating various agency services, and assessing the environment may be part of the care for the client with tuberculosis; however, these interventions are of less importance than education about the disease process and its treatment.
Question 46.
The nurse is reading the results of a tuberculin skin test (see figure). How should the nurse interpret the results?
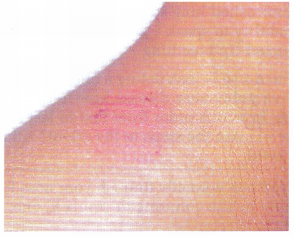
(a) negative
(b) needing to be repeated
(c) positive
(d) false
Answer:
(c) positive
Explanation:
The tuberculin test is positive. The test should be interpreted 2 to 3 days after administering the purified protein derivative (PPD) by measuring the size of the firm, raised area (induration). Positive responses indicate that the client may have been exposed to the tuberculosis bacteria. A negative response is indicated by the absence of a firm, raised area, or an area that is <5 mm in diameter. Since the test is positive, it is not necessary to redo the test. The test is positive, not false.
Question 47.
Which technique for administering the Mantoux test is correct?
(a) Hold the needle and syringe almost parallel to the client’s skin.
(b) Pinch the skin when inserting the needle.
(c) Aspirate before injecting the medication.
(d) Massage the site after injecting the medication.
Answer:
(a) Hold the needle and syringe almost parallel to the client’s skin.
Explanation:
The Mantoux test is administered via intradermal injection. The appropriate technique for an intradermal injection includes holding the needle and syringe almost parallel to the client’s skin, keeping the skin slightly taut when the needle is inserted, and inserting the needle with the bevel side up. There is no need to aspirate, a technique that assesses for incorrect placement in a blood vessel, when giving an intradermal injection. The injection site is not massaged.
Question 48.
A client had a Mantoux test result of an 8-mm induration. When should the nurse interpret the test as positive?
When the client:
(a) lives in a long-term care facility.
(b) has no known risk factors.
(c) is immunocompromised.
(d) works as a health care provider in a hospital.
Answer:
(c) is immunocompromised.
Explanation:
An induration (palpable raised hardened area of skin) of more than 5 to 15 mm (depending upon the person’s risk factors) to 10 Mantoux units is considered a positive result, indicating TB infection. An induration of >5 mm is found in HIV-positive individuals, those with recent contacts with persons with TB, persons with nodular or fibrotic changes on chest X-ray consistent with old healed TB, or clients with organ transplants or immunosup- pressed.
An induration of >10 mm is positive, and the client may be a recent arrival (<5 years) from high-prevalent countries, injection drug user, resident or an employee of high-risk congregate settings (e.g., prisons, long-term care facilities, hospitals, homeless shelters), or mycobacteriology lab personnel. An induration of >10 mm is also considered positive in persons with clinical conditions that place them at high risk (e.g., diabetes, prolonged corticosteroid therapy, leukemia, end-stage renal disease, chronic malabsorption syndromes, low body weight), a child <4 years of age, or a child or adolescents exposed to adults in high-risk categories.
Question 49.
Which family member exposed to tuberculosis would be at highest risk for contracting the disease?
(a) 45-year-old mother
(b) 17-year-old daughter
(c) 8-year-old son
(d) 76-year-old grandmother
Answer:
(d) 76-year-old grandmother
Explanation:
Older adults are believed to be at higher risk for contracting tuberculosis because of decreased immunocompetence. Other high-risk populations in the United States and Canada include the urban poor, clients with acquired immunodeficiency syndrome, and minority groups.
Question 50.
The nurse is teaching a client who has been diagnosed with tuberculosis how to avoid spreading the disease to family members. Which statements indicate that the client has understood the nurse’s instructions? Select all that apply.
(a) “I will need to dispose of my old clothing when I return home.”
(b) “I should always cover my mouth and nose when sneezing.”
(c) “It is important that I isolate myself from family when possible.”
(d) “I should use paper tissues to cough in and dispose of them promptly.”
(e) “I will avoid crowds.”
Answer:
(a) “I will need to dispose of my old clothing when I return home.”
(d) “I should use paper tissues to cough in and dispose of them promptly.”
Explanation:
(a), (c). When teaching the client how to avoid the transmission of tubercle bacilli, it is important for the client to understand that the organism is transmitted by droplet infection. Therefore, covering the mouth and nose when sneezing and using paper tissues to cough in with prompt disposal indicates that the client has understood the nurse’s instructions about preventing the spread of airborne droplets. It is not essential to discard clothing, nor does the client need to be isolated from family members. The client does not need to avoid crowds.
Question 51.
A client has a positive reaction to the Mantoux test. How should the nurse interpret this reaction?
The client has:
(a) active tuberculosis.
(b) been exposed to Mycobacterium tuberculosis.
(c) developed a resistance to tubercle bacilli.
(d) developed passive immunity to tuberculosis.
Answer:
(b) been exposed to Mycobacterium tuberculosis.
Explanation:
A positive Mantoux skin test indicates that the client has been exposed to tubercle bacilli. Exposure does not necessarily mean that active disease exists. A positive Mantoux test does not mean that the client has developed resistance. Unless involved in treatment, the client may still develop active disease at any time. Immunity to tuberculosis is not possible.
Question 52.
A client with tuberculosis is taking isoniazid (INH). What should the nurse instruct the client to do to help prevent development of peripheral neuropathies?
(a) Adhere to a low-cholesterol diet.
(b) Supplement the diet with pyridoxine (vitamin B6).
(c) Get extra rest.
(d) Avoid excessive sun exposure.
Answer:
(b) Supplement the diet with pyridoxine (vitamin B6).
Explanation:
INH competes for the available vitamin B6 in the body and leaves the client at risk for development of neuropathies related to vitamin deficiency. Supplemental vitamin B6 is routinely prescribed. Following a low-cholesterol diet, getting extra rest, and avoiding excessive sun exposure will not prevent the development of peripheral neuropathies.
Question 53.
The nurse is instructing a sexually active female who is taking isoniazid (INH). What should the nurse tell the client?
Isoniazid:
(a) increases the risk of vaginal infection.
(b) has mutagenic effects on ova.
(c) decreases the effectiveness of hormonal contraceptives.
(d) inhibits ovulation.
Answer:
(c) decreases the effectiveness of hormonal contraceptives.
Explanation:
INH interferes with the effectiveness of hormonal contraceptives, and female clients of childbearing age should be counseled to use an alternative form of birth control while taking the drug. INH does not increase the risk of vaginal infection, nor does it affect the ova or ovulation.
Question 54.
Clients who have had active tuberculosis are at risk for recurrence. Which condition increases that risk?
(a) cool and damp weather
(b) active exercise and exertion
(c) physical and emotional stress
(d) rest and inactivity
Answer:
(c) physical and emotional stress
Explanation:
Tuberculosis can be controlled but never completely eradicated from the body. Periods of intense physical or emotional stress increase the likelihood of recurrence. Clients should be taught to recognize the signs and symptoms of a potential recurrence. Weather and activity levels are not related to recurrences of tuberculosis.
Question 55.
In which areas of the United States and Canada is the incidence of tuberculosis highest?
(a) rural farming areas
(b) inner-city areas
(c) areas where clean water standards are low
(d) suburban areas with significant industrial pollution
Answer:
(b) inner-city areas
Explanation:
Statistics show that of the four geographic areas described, most cases of tuberculosis are found in inner-core residential areas of large cities, where health and sanitation standards tend to be low. Substandard housing, poverty, and crowded living conditions also generally characterize these city areas and contribute to the spread of the disease. Farming areas have a low incidence of tuberculosis. Variations in water standards and industrial pollution are not correlated to tuberculosis incidence.
Question 56.
A client who has been diagnosed with tuberculosis has been placed on drug therapy. The medication regimen includes rifampin. Which instruction should the nurse give the client about potential adverse effects of rifampin? Select all that apply.
(a) Have eye examinations every 6 months.
(b) Maintain follow-up monitoring of liver enzymes.
(c) Decrease protein intake in the diet.
(d) Avoid alcohol intake.
(e) The urine may have an orange color.
Answer:
(a) Have eye examinations every 6 months.
(d) Avoid alcohol intake.
(e) The urine may have an orange color.
Explanation:
(a), (d), (e). A potential adverse effect of rifampin is hepatotoxicity. Clients should be instructed to avoid alcohol intake while taking rifampin and keep follow-up appointments for periodic monitoring of liver enzyme levels to detect liver toxicity. Rifampin causes the urine to turn an orange color, and the client should understand that this is normal. It is not necessary to restrict protein intake in the diet or have the eyes examined due to rifampin therapy.
Question 57.
The nurse is providing follow-up care to a client with tuberculosis who does not regularly take the prescribed medication. Which nursing action would be most appropriate for this client?
(a) Ask the client’s spouse to supervise the daily administration of the medications.
(b) Visit the client weekly to verify compliance with taking the medication.
(c) Notify the health care provider (HCP) of the client’s noncompliance, and request a different prescription.
(d) Remind the client that tuberculosis can be fatal if it is not treated promptly.
Answer:
(a) Ask the client’s spouse to supervise the daily administration of the medications.
Explanation:
Directly observed therapy (DOT) can be implemented with clients who are not compliant with drug therapy. In DOT, a responsible person, who may be a family member or an HCP Q, observes the client taking the medication. Visiting the client, changing the prescription, or threatening the client will not ensure compliance if the client will not or cannot follow the prescribed treatment.
Question 58.
A client with newly diagnosed chronic obstructive disease is to be discharged home with oxygen per nasal prongs. Which teaching points should the nurse include in this client’s discharge plan? Select all that apply.
(a) Apply petroleum jelly on lips and nose to prevent dryness and irritation.
(b) Avoid areas where people are smoking cigarettes or cigars.
(c) Increase oxygen flow at night during hours of sleep.
(d) Place gauze between the ears and oxygen tubing to prevent skin irritation.
(e) Request a large, pressurized oxygen tank for use during car travel.
(f) Avoid use of a microwave oven when using oxygen.
Answer:
(b) Avoid areas where people are smoking cigarettes or cigars.
(d) Place gauze between the ears and oxygen tubing to prevent skin irritation.
Explanation:
(b), (d). Close proximity to smoking, fire, and small electrical appliances can be a fire hazard and should be avoided. The use of gauze is helpful in preventing skin irritation from the constant pressure and friction of the oxygen tubing. Typically, oxygen needs are lower at rest and during sleep. Increasing oxygen flow should be done at the discretion of the prescribing health care provider and not the client. Water-soluble lubricants are considered safer than petroleum-based lubricants. Small liquid oxygen tanks are easier to transport during travel than pressurized tanks. Use of microwave ovens for cooking is considered safe for those using supplemental oxygen.
Question 59.
Which information should the nurse include in a teaching plan for the client newly diagnosed with chronic obstructive pulmonary disease [COPD]? Select all that apply.
(a) Pulmonary rehabilitation programs offer very little benefit.
(b) Pneumococcal vaccination is contraindicated for clients with lung disease.
(c) High humidity increases the effort of breathing.
(d) A bronchodilator with metered-dose inhaler should be readily available.
(e) Smoking cessation is important to slow or stop disease progression.
Answer:
(c) High humidity increases the effort of breathing.
(d) A bronchodilator with metered-dose inhaler should be readily available.
(e) Smoking cessation is important to slow or stop disease progression.
Explanation:
(c), (d), (e). High humidity has been shown to increase the work of breathing. Carrying a metered- dose inhaler can facilitate early intervention if bronchospasm and shortness of breath should occur. Smoking cessation is difficult to achieve but very important in preventing COPD progression. Pulmonary rehabilitation programs are a great source of support for health promotion and maintenance for clients with COPD. Both the pneumococcal and influenza vaccines can help protect against respiratory infections.
Question 60.
A nurse is assessing a client with chronic emphysema. Which finding requires immediate intervention?
(a) using pursed-lip breathing and prolonged expiration
(b) circumoral cyanosis
(c) crackles auscultated posteriorly halfway up the left lung
(d) appearance of a “barrel chest”
Answer:
(c) crackles auscultated posteriorly halfway up the left lung
Explanation:
Crackles auscultated in the lung field indicate excessive fluid, a problem that requires immediate intervention. Pursed-lip breathing and a prolonged expiratory phase, circumoral cyanosis, and increased anterior-posterior diameter of the chest (resulting in “barrel chest”) are not unusual findings for clients with emphysema.
Question 61.
The nurse is assessing a client with chronic obstructive pulmonary disease. Which finding requires immediate intervention?
(a) distant heart sounds
(b) diminished lung sounds
(c) inability to speak
(d) pursed-lip breathing
Answer:
(c) inability to speak
Explanation:
Inability to speak could indicate respiratory distress. Pursed-lip breathing, while it is an abnormal finding, is not indicative of respiratory distress. Distant heart sounds could indicate heart failure but are not indicative of any distress. Diminished lung sounds may be normal for this client and do not require immediate intervention.
Question 62.
The nurse is instructing a client with chronic obstructive pulmonary disease how to do pursed-lip breathing. In which order from first to last should the nurse explain the steps to the client? All options must be used.
(a) “Breathe in normally through your nose for two counts (while counting to yourself, one, two).”
(b) “Relax your neck and shoulder muscles.”
(c) “Pucker your lips as if you were going to whistle.”
(d) “Breathe out slowly through pursed lips for four counts (while counting to yourself, one, two, three, four).”
Answer:
(b) “Relax your neck and shoulder muscles.”
(a) “Breathe in normally through your nose for two counts (while counting to yourself, one, two).”
(c) “Pucker your lips as if you were going to whistle.”
(d) “Breathe out slowly through pursed lips for four counts (while counting to yourself, one, two, three, four).”
Explanation:
(b), (a), (c), (d). The nurse should first instruct the client to relax the neck and the shoulders and then take several normal breaths. After taking a breath in, the client should pucker the lips and finally breathe out through pursed lips.
Question 63.
The nurse reviews an arterial blood gas report for a client with chronic obstructive pulmonary disease (COPD). The results are as follows: pH 7.35; PCO2 62 (8.25 kPa); PO2 70 (9.31 kPa); HCO3 34 mEq/L (34 mmol/L). What should the nurse do first?
(a) Apply a 100% nonrebreather mask.
(b) Assess the vital signs.
(c) Reposition the client.
(d) Prepare for intubation.
Answer:
(b) Assess the vital signs.
Explanation:
Clients with chronic COPD have CO2 retention, and the respiratory drive is stimulated when the PO2 decreases. The heart rate, respiratory rate, and blood pressure should be evaluated to determine if the client is hemodynamically stable. Symptoms, such as dyspnea, should also be assessed. After assessing the vital signs, the nurse should assist the client as needed to assume the most comfortable position for breathing. Oxygen supplementation, if indicated, should be titrated upward in small increments. There is no indication that the client is experiencing respiratory distress requiring intubation.
Question 64.
When developing a discharge plan with a client with chronic obstructive pulmonary disease (COPD), what information should the nurse include in the plan?
People with COPD:
(a) develop respiratory infections easily.
(b) usually maintain their current status.
(c) require less supplemental oxygen.
(d) show permanent improvement.
Answer:
(a) develop respiratory infections easily.
Explanation:
A client with COPD is at high risk for development of respiratory infections. COPD is slowly progressive; therefore, maintaining current status and establishing a goal that the client will require less supplemental oxygen are unrealistic expectations. Treatment may slow progression of the disease, but permanent improvement is highly unlikely.
Question 65.
The client with chronic obstructive pulmonary disease is taking theophylline. The nurse should instruct the client to report which signs of theophylline toxicity? Select all that apply.
(a) nausea
(b) vomiting
(c) seizures
(d) insomnia
(e) vision changes
Answer:
(a) nausea
(b) vomiting
(c) seizures
(d) insomnia
Explanation:
(a), (b), (c), (d). The therapeutic range for serum theophylline is 10 to 20 mcg/mL (55.5 to 111 pmol/L). At higher levels, the client will experience signs of toxicity such as nausea, vomiting, seizures, and insomnia. The nurse should instruct the client to report these signs and to keep appointments to have theophylline blood levels monitored. If the theophylline level is below the therapeutic range, the client may be at risk for more frequent exacerbations of the disease.
Question 66.
Which statement indicates that the client with chronic obstructive pulmonary disease (COPD) who has been discharged to home understands the care plan?
The client:
(a) plans to avoid direct contact with family and friends.
(b) can state actions to reduce pain.
(c) will use oxygen via a nasal cannula at 5 L/min.
(d) agrees to call the health care provider (HCP) if dyspnea on exertion increases.
Answer:
(d) agrees to call the health care provider (HCP) if dyspnea on exertion increases.
Explanation:
Increasing dyspnea on exertion indicates that the client may be experiencing complications of COPD. Therefore, the client should notify the HCP It is not necessary to avoid being around others. Pain is not a common symptom of COPD. Clients with COPD use low-flow oxygen supplementation (1 to 2 L/min) to avoid suppressing the respiratory drive, which, for these clients, is stimulated by hypoxia.
Question 67.
When instructing clients on how to decrease the risk of developing chronic obstructive pulmonary disease (COPD), the nurse should emphasize which instruction?
(a) Participate regularly in aerobic exercises.
(b) Maintain a high-protein diet.
(c) Avoid exposure to people with known respiratory infections.
(d) Abstain from cigarette smoking.
Answer:
(d) Abstain from cigarette smoking.
Explanation:
Cigarette smoking is the primary cause of COPD. Other risk factors include exposure to environmental pollutants and chronic asthma. Participating in an aerobic exercise program, although beneficial, will not decrease the risk of COPD. Insufficient protein intake and exposure to people with respiratory infections do not increase the risk of COPD.
Question 68.
The nurse is instructing the client with chronic obstructive pulmonary disease to do pursed-lip breathing. What is the expected outcome of this exercise?
(a) improved oxygen intake
(b) deeper diaphragmatic breathing
(c) stronger intercostal muscles
(d) better elimination of carbon dioxide
Answer:
(d) better elimination of carbon dioxide
Explanation:
Pursed-lip breathing prolongs exhalation and prevents air trapping in the alveoli, thereby promoting carbon dioxide elimination. By prolonging exhalation and helping the client relax, pursed-lip breathing helps the client learn to control the rate and depth of respiration. Pursed-lip breathing does not promote the intake of oxygen, strengthen the diaphragm, or strengthen intercostal muscles.
Question 69.
Which is a priority goal for the client with chronic obstructive pulmonary disease (COPD)?
(a) maintaining functional ability
(b) minimizing chest pain
(c) increasing carbon dioxide levels in the blood
(d) treating infectious agents
Answer:
(a) maintaining functional ability
Explanation:
A priority goal for the client with COPD is to manage the signs and symptoms of the disease process so as to maintain the client’s functional ability. Chest pain is not a typical symptom of COPD. The carbon dioxide concentration in the blood is increased to an abnormal level in clients with COPD; it would not be a goal to increase the level further. Preventing infection would be a goal of care for the client with COPD.
Question 70.
When teaching a client with chronic obstructive pulmonary disease to conserve energy to conserve energy, what instruction should the nurse give the client about breathing when lifting heavy objects?
Lift the object by:
(a) inhaling through an open mouth.
(b) exhaling through pursed lips.
(c) exhaling but before inhaling.
(d) taking a deep breath and holding it.
Answer:
(b) exhaling through pursed lips.
Explanation:
Exhaling requires less energy than does inhaling. Therefore, lifting while exhaling saves energy and reduces perceived dyspnea. Pursing the lips prolongs exhalation and provides the client with more control over breathing. Lifting after exhaling but before inhaling is similar to lifting with the breath held. This should not be recommended because it is similar to Valsalva’s maneuver, which can stimulate cardiac arrhythmias.

Question 71.
The nurse is teaching a client with chronic obstructive pulmonary disease (COPD) to assess for signs and symptoms of right-sided heart failure. Which signs and symptoms should be included in the teaching plan?
(a) clubbing of nail beds
(b) hypertension
(c) peripheral edema
(d) increased appetite
Answer:
(c) peripheral edema
Explanation:
Right -sided heart failure is a complication of COPD that occurs because of pulmonary hypertension. Signs and symptoms of right-sided heart failure include peripheral edema, jugular venous distention, hepatomegaly, and weight gain due to increased fluid volume. Clubbing of nail beds is associated with conditions of chronic hypoxemia. Hypertension is associated with left-sided heart failure. Clients with heart failure have decreased appetites.
Question 72.
The nurse is assessing the respiratory status of a client who is experiencing an exacerbation of chronic obstructive pulmonary disease (COPD) secondary to an upper respiratory tract infection. Which finding is expected?
(a) normal breath sounds
(b) prolonged inspiration
(c) normal chest movement
(d) coarse crackles and rhonchi
Answer:
(d) coarse crackles and rhonchi
Explanation:
Exacerbations of COPD are commonly caused by respiratory infections. Coarse crackles and rhonchi would be auscultated as air moves through airways obstructed with secretions. In COPD, breath sounds are diminished because of an enlarged anteroposterior diameter of the chest. Expiration, not inspiration, becomes prolonged. Chest movement is decreased as lungs become overdistended.
Question 73.
A client with chronic obstructive pulmonary disease (COPD) is experiencing dyspnea and has a low Pa02 level. The nurse plans to administer oxygen as prescribed. Which statement is true concerning oxygen administration to a client with COPD?
(a) High oxygen concentrations will cause coug h ing and dyspnea.
(b) High oxygen concentrations may inhibit thehypoxic stimulus to breathe.
(c) Increased oxygen use will cause the client to become dependent on the oxygen.
(d) Administration of oxygen is contraindicated in clients who are using bronchodilators.
Answer:
(b) High oxygen concentrations may inhibit thehypoxic stimulus to breathe.
Explanation:
Clients who have a long history of COPD may retain carbon dioxide (CO2). Gradually, the body adjusts to the higher CO2 concentration, and the high levels of CO2 no longer stimulate the respiratory center. The major respiratory stimulant then becomes hypoxemia. Administration of high concentrations of oxygen eliminates this respiratory stimulus and leads to hypoventilation. Oxygen can be drying if it is not humidified, but it does not cause coughing and dyspnea. Increased oxygen use will not create an oxygen dependency; clients should receive oxygen as needed. Oxygen is not contraindicated with the use of bronchodilators.
Question 74.
Which diet would be most appropriate for a client with chronic obstructive pulmonary disease (COPD)?
(a) low-fat, low-cholesterol diet
(b) bland, soft diet
(c) low-sodium diet
(d) high-calorie, high-protein diet
Answer:
(d) high-calorie, high-protein diet
Explanation:
The client should eat high-calorie, high-protein meals to maintain nutritional status and prevent weight loss that results from the increased work of breathing. The client should be encouraged to eat small, frequent meals. A low-fat, low-cholesterol diet is indicated for clients with coronary artery disease. The client with COPD does not necessarily need to follow a sodium- restricted diet, unless otherwise medically indicated. There is no need for the client to eat bland, soft foods.
Question 75.
The nurse administers theophylline to a client. When evaluating the effectiveness of this medication, what is an expected outcome?
(a) suppression of the client’s respiratory infection
(b) decrease in bronchial secretions
(c) less difficulty breathing
(d) thinning of tenacious, purulent sputum
Answer:
(c) less difficulty breathing
Explanation:
Theophylline is a bronchodilator that is administered to relax airways and decrease dyspnea. Theophylline is not used to treat infections and does not decrease or thin secretions.
Question 76.
The nurse is planning to teach a client with chronic obstructive pulmonary disease how to cough effectively. Which instruction should be included?
(a) Take a deep abdominal breath, bend forward, and cough three or four times on exhalation.
(b) Lie flat on the back, splint the thorax, take two deep breaths, and cough.
(c) Take several rapid, shallow breaths, and then cough forcefully.
(d) Assume a side-lying position, extend the arm over the head, and alternate deep breathing with coughing.
The Client with Asthma
Answer:
(a) Take a deep abdominal breath, bend forward, and cough three or four times on exhalation.
Explanation:
The goal of effective coughing is to conserve energy, facilitate removal of secretions, and minimize airway collapse. The client should assume a sitting position with feet on the floor if possible. The client should bend forward slightly and, using pursed-lip breathing, exhale. After resuming an upright position, the client should use abdominal breathing to slowly and deeply inhale.
After repeating this process three or four times, the client should take a deep abdominal breath, bend forward, and cough three or four times upon exhalation (“huff” cough). Lying flat does not enhance lung expansion; sitting upright promotes full expansion of the thorax. Shallow breathing does not facilitate removal of secretions, and forceful coughing pro-motes collapse of airways. A side-lying position does not allow for adequate chest expansion to promote deep breathing.
Question 77.
The nurse observes a client using a metered- dose inhaler (MDI) to aid in management of asthma. Which actions indicate that the client needs further instruction? Select all that apply.
(a) shakes the MDI before using
(b) exhales before starting to use the MDI
(c) inspires rapidly when dispensing the medication from the MDI
(d) holds the breath for 3 seconds after inhaling with the MDI
(e) cleans the inhaler and canister in soapy water before using again in rapid succession
Answer:
(c) inspires rapidly when dispensing the medication from the MDI
(d) holds the breath for 3 seconds after inhaling with the MDI
(e) cleans the inhaler and canister in soapy water before using again in rapid succession
Explanation:
(c), (d), (e). Utilization of an MDI requires the following actions: shaking the MDI before use; exhaling prior to dispensing the medication; taking a deep breath to ensure the medication is distributed in the lungs and holding it for 10 seconds or as long as possible to disperse the medication into the lungs; and allowing 30 seconds between puffs to provide an adequate amount of inhalation medication. The client should rinse the plastic parts of the MDI and wipe them dry; the canister should not become wet.
Question 78.
A client with a history of asthma is admitted to the emergency department. The nurse notes that the client is dyspneic, with a respiratory rate of 35 breaths/min, nasal flaring, and use of accessory muscles. Auscultation of the lung fields reveals greatly diminished breath sounds. What should the nurse do first?
(a) Initiate oxygen therapy as prescribed, and reassess the client in 10 minutes.
(b) Draw blood for an arterial blood gas.
(c) Encourage the client to relax and breathe slowly through the mouth.
(d) Administer bronchodilators as prescribed.
Answer:
(d) Administer bronchodilators as prescribed.
Explanation:
In an acute asthma attack, diminished or absent breath sounds can be an ominous sign indicating lack of air movement in the lungs and impending respiratory failure. The client requires immediate intervention with inhaled bronchodila- tors, IV corticosteroids, and, possibly, IV theophylline. Administering oxygen and reassessing the client 10 minutes later would delay needed medical intervention, as would drawing blood for an arterial blood gas analysis. It would be futile to encourage the client to relax and breathe slowly without providing the necessary pharmacologic intervention.
Question 79.
A client is experiencing an acute asthmatic attack. Prior to treatment with levalb- uterol, respirations were 40 breaths/min, pulse 132 beats/min, oxygen saturation 86% on room air, and there was audible wheezing. Which finding indicates achievement of the desired outcome of asthma treatment?
(a) decreased peak expiratory flow (PEF) rate
(b) wheezing inaudible with diminished breath sounds
(c) pulse 96 bpm and SpO2 92% on room air
(d) inspiratory cycle twice as long as the expiratory cycle
Answer:
(c) pulse 96 bpm and SpO2 92% on room air
Explanation:
Quick-acting bronchodilators are used in acute asthma to improve airflow and relieve symptoms; following treatment, tachycardia resolves as gas exchange and work of breathing are improved. SpO2 and PEF rates improve, and wheezing from a constricted airway resolves. The normal inspiratory to expiratory ratio is 1:2.
Question 80.
For a client with asthma, the health care provider (HCP) prescribes albuterol, two puffs twice a day via a metered-dose inhaler (MDI), and beclometh- asone, two puffs twice a day via MDI. How should the nurse instruct the client to administer these drugs?
(a) “Take the medications 1 hour apart, two times a day.”
(b) “Take the albuterol first and follow with beclomethasone two times a day.”
(c) “Take the albuterol on awakening and alternate the medications every 4 hours.”
(d) “Take the beclomethasone inhaler first and follow with albuterol.”
Answer:
(b) “Take the albuterol first and follow with beclomethasone two times a day.”
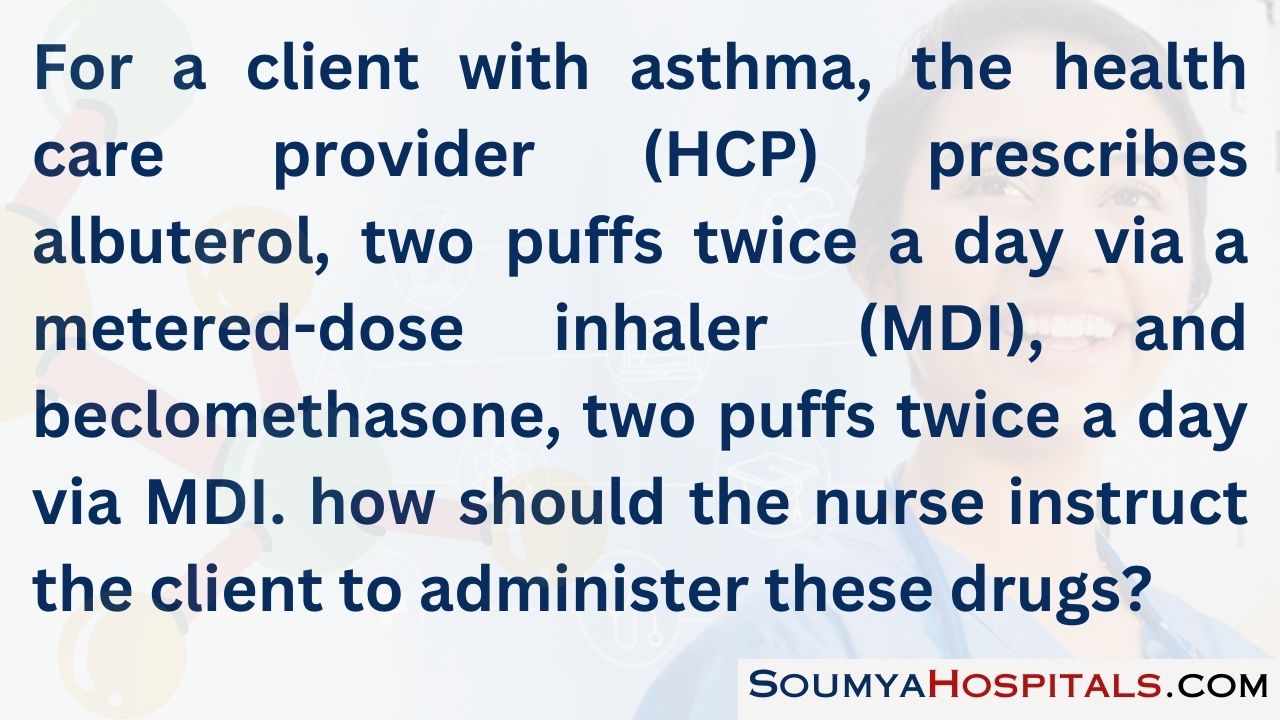
Explanation:
The nurse instructs the client to administer the bronchodilator first (the beta-2 agonist always leads) in order to open the airway and allow for improved delivery of the corticosteroid to the lung tissue, which follows after 1 minute between puffs. Using a spacer device with an MDI provides the best delivery of medication to the lungs.
Question 81.
A client experiencing a severe asthma attack has the following arterial blood gas results: pH 7.33; PCO2 48 mm Hg (6.4 kPa); P02 58 mm Hg (7.7 kPa); HCO3 26 mEq/L (26 mmol/L). Which prescription should the nurse implement first?
(a) albuterol nebulizer
(b) chest X-ray
(c) ipratropium inhaler
(d) sputum culture
Answer:
(a) albuterol nebulizer
Explanation:
The arterial blood gas reveals a respiratory acidosis with hypoxia. A quick-acting bronchodilator, albuterol, should be administered via nebulizer to improve gas exchange. Ipratropium is a maintenance treatment for bronchospasm that can be used with albuterol. A chest X-ray and sputum sample can be obtained once the client is stable.
Question 82.
The nurse is instructing a client with acute asthma who is taking short-term corticosteroid therapy. The nurse should tell the client that steroids will have which expected outcome?
Steroids will:
(a) promote bronchodilation.
(b) act as an expectorant.
(c) have an anti-inflammatory effect.
(d) prevent development of respiratory infections.
Answer:
(c) have an anti-inflammatory effect.
Explanation:
Corticosteroids have an anti-inflammatory effect and act to decrease edema in the bronchial airways and decrease mucus secretion. Corticosteroids do not have a bronchodilator effect, act as expectorants, or prevent respiratory infections.
Question 83.
The nurse is teaching the client how to use a metered-dose inhaler (MDI) to administer a corticosteroid. Which observation indicates that the client is using the MDI correctly? Select all that apply.
(a) The inhaler is held upright.
(b) The head is tilted down while inhaling the medicine.
(c) The client waits 5 minutes between puffs.
(d) The client rinses the mouth with water following administration.
(e) The client lies supine for 15 minutes following administration.
Answer:
(a) The inhaler is held upright.
(d) The client rinses the mouth with water following administration.
Explanation:
(a), (d). The client should shake the inhaler and hold it upright when administering the drug. The head should be tilted back slightly. The client should wait about 30 seconds between puffs. The mouth should be rinsed following the use of a corticosteroid MDI to decrease the likelihood of developing an oral infection. The client does not need to lie supine; instead, the client will likely to be able to breathe more freely if sitting upright.
Question 84.
A client is prescribed metaproterenol via a metered-dose inhaler, two puffs every 4 hours. The nurse instructs the client to report which adverse effect?
(a) irregular heartbeat
(b) constipation
(c) pedal edema
(d) decreased pulse rate
Answer:
(a) irregular heartbeat
Explanation:
Irregular heartbeats should be reported promptly to the care provider. Metaproterenol may cause irregular heartbeat, tachycardia, or anginal pain because of its adrenergic effect on beta-adrenergic receptors in the heart. It is not recommended for use in clients with known cardiac disorders. Metaproterenol does not cause constipation, pedal edema, or bradycardia.
Question 85.
A client who has been taking flunisolide nasal spray, two inhalations a day, for treatment of asthma has painful, white patches in the mouth. What should the nurse tell the client?
(a) “This is an anticipated adverse effect of your medication. It should go away in a couple of weeks.”
(b) “You are using your inhaler too much, and it has irritated your mouth.”
(c) “You have developed a fungal infection from your medication. It will need to be treated with an antifungal agent.”
(d) “Be sure to brush your teeth and floss daily. Good oral hygiene will treat this problem.”
Answer:
(c) “You have developed a fungal infection from your medication. It will need to be treated with an antifungal agent.”
Explanation:
Use of oral inhalant corticosteroids such as flunisolide can lead to the development of oral thrush, a fungal infection. Once developed, thrush must be treated by antifungal therapy; it will not resolve on its own. Fungal infections can develop even without overuse of the corticosteroid inhaler. Although good oral hygiene can help prevent development of a fungal infection, it cannot be used alone to treat the problem.
Question 86.
A nurse is teaching a client to use a metered- dose inhaler (MDI) to administer bronchodilator medication. Indicate the correct order of the steps from first to last the client should take to use the MDI appropriately. All options must be used.
(a) Shake the inhaler immediately before use.
(b) Hold the breath for 10 seconds, and then exhale.
(c) Activate the MDI on inhalation.
(d) Breathe out through the mouth.
Answer:
(a) Shake the inhaler immediately before use.
(d) Breathe out through the mouth.
(c) Activate the MDI on inhalation.
(b) Hold the breath for 10 seconds, and then exhale.
Explanation:
(a), (d), (c), (b). When using inhalers, clients should first shake the inhaler to activate the MDI and then breathe out through the mouth. Next, the client should activate the MDI while inhaling, hold the breath for 5 to 10 seconds, and then exhale normally.
Question 87.
Which instruction should the nurse include in the discharge teaching plan for a client with asthma? Select all that apply.
(a) Incorporate physical exercise as tolerated into the daily routine.
(b) Monitor peak flow numbers after meals and at bedtime.
(c) Eliminate stressors in the work and home environment.
(d) Use melatonin to ensure uninterrupted sleep at night.
(e) Avoid smoke-filled rooms.
Answer:
(a) Incorporate physical exercise as tolerated into the daily routine.
(e) Avoid smoke-filled rooms.
Explanation:
(a), (e). Physical exercise is beneficial and should be incorporated as tolerated into the client’s schedule. The client should also avoid areas with smoke, as smoke is a trigger for an asthma attack. Peak flow numbers should be monitored daily, usually in the morning (before taking medication). Peak flow does not need to be monitored after each meal. Stressors in the client’s life should be modified but cannot be totally eliminated. Although adequate sleep is important, it is not recommended that a drug such as melatonin or sedatives be routinely taken to induce sleep.
Question 88.
The nurse should teach the client with asthma to avoid which of the most common precipitating factors of an acute asthma attack?
(a) occupational exposure to toxins
(b) Valsalva’s maneuver
(c) exposure to cigarette smoke
(d) exercising in cold temperatures
Answer:
(c) exposure to cigarette smoke
Explanation:
A common precipitator of asthma attacks is exposure to cigarette and cigar smoke. The client should avoid being in environments where there is exposure to smoke. Environmental exposure to toxins or heavy particulate matter can trigger asthma attacks; however, far fewer asthmatics are exposed to such toxins than are exposed to smoke. Valsalva’s maneuver (holding the breath while defecating or bearing down) is associated with causing cardiac arrhythmias. Rarely, asthmatic attacks are triggered by exercising in cold weather.
Question 89.
When assessing a client with asthma, which findings would most likely indicate the presence of a respiratory infection?
(a) cough productive of yellow sputum
(b) bilateral expiratory wheezing
(c) chest tightness
(d) respiratory rate of 30 breaths/min
Answer:
(a) cough productive of yellow sputum
Explanation:
A cough productive of yellow sputum is the most likely indicator of a respiratory infection. The other signs and symptoms-wheezing, chest tightness, and increased respiratory rate-are all findings associated with an asthma attack and do not necessarily mean an infection is present.
Question 90.
The nurse has assisted the health care provider at the bedside with insertion of a left subclavian, triple lumen catheter in a client admitted with lung cancer. Suddenly, the client becomes restless and tachypneic. What should the nurse do next?
(a) Assess breath sounds.
(b) Remove the catheter.
(c) Insert a peripheral IV.
(d) Reposition the client.
Answer:
(a) Assess breath sounds.
Explanation:
The nurse should first assess for bilateral breath sounds since a complication of central line insertion is a pneumothorax, which would cause an increase in respiratory rate and drop in oxygen, causing irritability. The nurse should also assess blood pressure and heart rate for the complication of bleeding. A chest X-ray will be performed to determine correct placement and complications. A central line was most likely placed because peripheral IV access was not available or adequate for the client. Repositioning may be considered after assessments are done.
Question 91.
A client who has been recently extubated has shortness of breath. The nurse reports the client’s discomfort and the results of the recently prescribed arterial blood gas analysis to the health care provider (HCP). After reviewing the report of the complete blood count (see report), the nurse should also report which results to the HCP?
(a) prothrombin time (PT)
(b) hemoglobin and hematocrit
(c) monocytes
(d) platelets
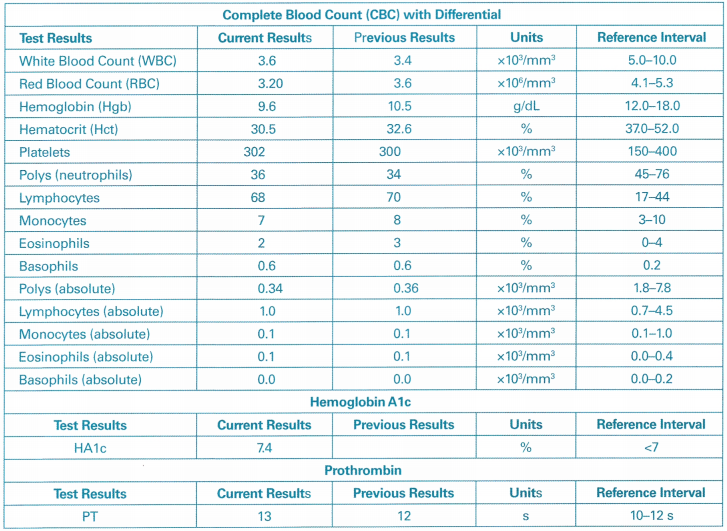
Answer:
(b) hemoglobin and hematocrit
Explanation:
The nurse should review the CBC with differential to evaluate the client’s hemoglobin and hematocrit, which are abnormal and should be reported to the HCP. Anemia leads to decreased oxygen-carrying capacity of the blood. A client unable to compensate for the anemia may experi-ence a profound sense of dyspnea. There has been a significant drop in the hemoglobin and hematocrit since the previous report, and these should be reported to the HCP. The monocytes are within normal range. AtC is a laboratory test evaluating glycosylated hemoglobin and is in the normal range. This test is used to diagnose diabetes and/or monitor diabetic glucose control over time. PT is a coagulation study reflecting liver function and clotting time and is in the normal range.
Question 92.
A female client diagnosed with lung cancer is to have a left lower lobectomy. The nurse should assess the client for which factor that increases the client’s risk of developing postoperative pulmonary complications?
(a) Height is 5 feet, 7 inches (170.2 cm) and weight is 110 lb (49.9 kg).
(b) The client tends to keep her real feelings to herself.
(c) She ambulates and can climb one flight of stairs without dyspnea.
(d) The client is 58 years of age.
Answer:
(a) Height is 5 feet, 7 inches (170.2 cm) and weight is 110 lb (49.9 kg).
Explanation:
Risk factors for postoperative pulmonary complications include malnourishment, which is indicated by this client’s height and weight. It is thought that emotional responses can affect overall health; however, not verbalizing one’s feelings is not a contributing factor in postoperative pulmo-nary complications. The client’s current activity level and age do not place her at increased risk for complications.
Question 93.
The nurse is preparing a client for surgery and notices that the client looks sad. The client says, “I am scared of having cancer. It is so horrible, and I brought it on myself. I should have quit smoking years ago.” What would be the nurse’s best response to the client?
(a) “It’s okay to be scared. What is it about cancer that you are afraid of?”
(b) “It’s normal to be scared. I would be, too. We will help you through it.”
(c) “Don’t be so hard on yourself. You don’t know if your smoking caused the cancer.”
(d) “Do you feel guilty because you smoked?”
Answer:
(a) “It’s okay to be scared. What is it about cancer that you are afraid of?”
Explanation:
Acknowledging the basic feeling the client expresses—fear—and asking an open-ended question allow the client to explain any fears. The other options dismiss the client’s feelings and may give false reassurance or label the client’s feelings. The client should be encouraged to explore feelings about a cancer diagnosis.
Question 94.
A client who underwent a left lower lobectomy has been out of surgery for 48 hours. The client is receiving morphine sulfate via a patient- controlled analgesia (PCA) system and reports having pain in the left thorax that worsens when coughing. After checking the PCA system, what should the nurse do next?
(a) Let the client rest so the client is not stimulated to cough.
(b) Encourage the client to take deep breaths to help control the pain.
(c) Reassure the client that the machine is working and will administer medication to relieve the pain.
(d) Obtain a more detailed assessment of the client’s pain using a pain scale.
Answer:
(d) Obtain a more detailed assessment of the client’s pain using a pain scale.
Explanation:
Systematic pain assessment is necessary for adequate pain management in the postoperative client. Guidelines from a variety of health care agencies and nursing groups recommend that institutions adopt a pain assessment scale to assist in facilitating pain management. Even though the client is receiving morphine sulfate by PCA, and the pump is working, the nurse should continue to assess the client. The concern is not to eliminate coughing but to control pain adequately. Coughing is necessary to prevent postoperative atelectasis and pneumonia. Breathing exercises may help control pain in some circumstances; however, most clients with thoracic surgery require parenteral opioid analgesics in the early postoperative period. Although it is necessary that the PCA device be checked periodically, reassuring the client is not sufficient, so further assessment is needed.
Question 95.
Which factor is a priority for the nurse to evaluate when completing discharge planning for a client who has had a lobectomy for treatment of lung cancer?
(a) the support available to assist the client at home
(b) the distance the client lives from the hospital
(c) the client’s ability to do home blood pressure monitoring
(d) the client’s knowledge of the causes of lung cancer
Answer:
(a) the support available to assist the client at home
Explanation:
Because clients are discharged as soon as possible from the hospital, it is essential to evaluate the support they have to assist them with self-care at home. The distance the client lives from the hospital is not a critical factor in discharge planning. There are no data indicating that home blood pressure monitoring is needed. Knowledge of the causes of lung cancer, although important, is not the most essential area to evaluate given the client’s postoperative status.
Question 96.
After a thoracotomy, the nurse instructs the client to perform deep-breathing exercises. What is an expected outcome of these exercises?
(a) The elevated diaphragm enlarges the thorax and increases the lung surface available for gas exchange.
(b) There is increased blood flow to the lungs to allow them to recover from the trauma of surgery.
(c) The rate of airflow to the remaining lobe is controlled so that it will not become hyperinflated.
(d) The alveoli expand and increase the lung surface available for ventilation.
Answer:
(d) The alveoli expand and increase the lung surface available for ventilation.
Explanation:
Deep breathing helps prevent microatelectasis and pneumonitis and also helps force air and fluid out of the pleural space into the chest tubes. More than half of the ventilatory process is accomplished by the rise and fall of the diaphragm. The diaphragm is the major muscle of respiration; deep breathing causes it to descend, not elevate, thereby increasing the ventilating surface. Deep breathing increases blood flow to the lungs; however, the primary reason for deep breathing is to expand alveoli and prevent atelectasis. The remaining lobe naturally hyperinflates to fill the space created by the resected lobe. This is an expected phenomenon.
Question 97.
Following a thoracotomy, the client has pain of 9 on a 10-point scale. What should the nurse do thirty minutes after administering the highest dose of the prescribed pain medication?
(a) Reposition the client.
(b) Reassess the client.
(c) Reassure the client.
(d) Readjust the pain medication dosage as needed.
Answer:
(b) Reassess the client.
Explanation:
It is essential that the nurse evaluate the effects of pain medication after the medication has had time to act; reassessment is necessary to determine the effectiveness of the pain management plan. Although it is prudent to check for discomfort related to positioning when assessing the client’s pain, repositioning the client immediately after administering pain medication is not necessary. Verbally reassuring the client after administering pain medication may be useful to help instill confidence in the treatment plan; however, it is not as important as evaluating the effectiveness of the medication. Readjusting the pain medication dosage as needed according to the client’s condition is essential, but the effectiveness of the medication must be evaluated first.
Question 98.
While assessing a thoracotomy incisional area from which a chest tube exits, the nurse feels a crackling sensation under the fingertips along the entire incision. What should the nurse do next?
(a) Lower the head of the bed, and call the health care provider (HCP).
(b) Prepare an aspiration tray.
(c) Mark the area with a skin pencil at the outer periphery of the crackling.
(d) Turn off the suction of the chest drainage system.
Answer:
(c) Mark the area with a skin pencil at the outer periphery of the crackling.
Explanation:
This crackling sensation is subcutaneous emphysema. Subcutaneous emphysema is not an unusual finding and is not dangerous if confined, and the nurse should mark the area to detect if the area is expanding. Progression can be serious, especially if the neck is involved; a tracheotomy may be needed at that point. If emphysema progresses noticeably in 1 hour, the HCP should be notified. Lowering the head of the bed will not arrest the progress or provide any further information. A tracheotomy tray would be useful if subcutaneous emphysema progresses to the neck. Subcutaneous emphysema may progress if the chest drainage system does not adequately remove air and fluid; therefore, the system should not be turned off.
Question 99.
When teaching a client to deep breathe effectively after a lobectomy, what should the nurse instruct the client to do?
(a) Contract the abdominal muscles; take a slow, deep breath through the nose; hold it for 3 to 5 seconds; and then exhale.
(b) Contract the abdominal muscles, take a deep breath through the mouth, and exhale slowly as if trying to blow out a candle.
(c) Relax the abdominal muscles; take a slow, deep breath through the nose; and hold it for 3 to 5 seconds.
(d) Relax the abdominal muscles, take a deep breath through the mouth, and exhale slowly over 10 seconds.
Answer:
(a) Contract the abdominal muscles; take a slow, deep breath through the nose; hold it for 3 to 5 seconds; and then exhale.
Explanation:
The recommended procedure for teaching clients postoperatively to deep breathe includes contracting (pulling in) the abdominal muscles and taking a slow, deep breath through the nose. This breath is held 3 to 5 seconds, which facilitates alveolar ventilation by improving the inspiratory phase of ventilation. Exhaling slowly as if trying to blow out a candle is a technique used in pursed- lip breathing to facilitate exhalation in clients with chronic obstructive pulmonary disease. It is recommended that the abdominal muscles be contracted, not relaxed, to promote deep breathing. The client should breathe through the nose.
Question 100.
Which instruction should the nurse give the client who has undergone chest surgery to prevent shoulder ankylosis?
(a) Turn from side to side.
(b) Raise and lower the head.
(c) Raise the arm on the affected side over the head.
(d) Flex and extend the elbow on the affected side.
Answer:
(c) Raise the arm on the affected side over the head.
Explanation:
A client who has undergone chest surgery should be taught to raise the arm on the affected side over the head to help prevent shoulder ankylosis. This exercise helps restore normal shoulder movement, prevents stiffening of the shoulder joint, and improves muscle tone and power. Turning from side to side, raising and lowering the head, and flexing and extending the elbow on the affected side do not exercise the shoulder joint.
Question 101.
A client has a chest tube and water seal drainage system. What should the nurse do to ensure safe and effective use of the drainage system?
(a) Verify that the air vent on the water seal drainage system is capped when the suction is off.
(b) Strip the chest drainage tubes at least every 4 hours if excessive bleeding occurs.
(c) Ensure that the chest tube is clamped when moving the client out of the bed.
(d) Make sure that the drainage apparatus is always below the client’s chest level.
Answer:
(d) Make sure that the drainage apparatus is always below the client’s chest level.
Explanation:
The drainage apparatus is always kept below the client’s chest level to prevent backflow of fluid into the pleural space. The air vent must always be open in the closed chest drainage system to allow air from the client to escape. Stripping a chest tube causes excessive negative intrapleural pressure and is not recommended. Clamping a chest tube when moving a client is not recommended.
Question 102.
A client has a chest tube attached to a water seal drainage system, and the nurse notes that the fluid in the chest tube and in the water seal column has stopped fluctuating. How should the nurse interpret this finding?
(a) The lung has fully expanded.
(b) The lung has collapsed.
(c) The chest tube is in the pleural space.
(d) The mediastinal space has decreased.
Answer:
(a) The lung has fully expanded.
Explanation:
Cessation of fluid fluctuation in the tubing can mean one of several things: the lung has fully expanded and negative intrapleural pressure has been reestablished, the chest tube is occluded, or the chest tube is not in the pleural space. Fluid fluctuation occurs because during inspiration, intrapleural pressure exceeds the negative pressure generated in the water seal system. Therefore, drainage moves toward the client. During expiration, the pleural pressure exceeds that generated in the water seal system, and fluid moves away from the client. When the lung is collapsed or the chest tube is in the pleural space, fluid fluctuation is likely to be noted. The chest tube is not inserted in the mediastinal space.
Question 103.
The nurse observes a constant gentle bubbling in the water seal column of a water seal chest drainage system. What should the nurse do next?
(a) Continue monitoring as usual; this isexpected.
(b) Check the connectors between the chest and drainage tubes and where the drainage tube enters chest drainage system.
(c) Decrease the suction and continue observing the system for changes in bubbling during the next several hours.
(d) Notify the health care provider (HCP).
Answer:
(b) Check the connectors between the chest and drainage tubes and where the drainage tube enters chest drainage system.
Explanation:
There should never be constant bubbling in the water seal system; normally, the bubbling is intermittent. Constant bubbling in the water seal bottle indicates an air leak, which means that less negative pressure is being exerted on the pleural space. Decreasing the suction will not reduce the leak. It is not necessary to notify the HCP Q until the system has been checked and the problem identified.
Question 104.
A client who underwent a lobectomy and has a water seal chest drainage system is breathing with a little more effort and at a faster rate than 1 hour ago. The client’s pulse rate is also increased. What should the nurse do next?
(a) Check the tubing to ensure that the client is not lying on it or kinking it.
(b) Increase the suction.
(c) Lower the drainage bottles 2 to 3 feet (61 to 91.4 cm) below the level of the client’s chest.
(d) Ensure that the chest tube has two clamps on it to prevent air leaks.
Answer:
(a) Check the tubing to ensure that the client is not lying on it or kinking it.
Explanation:
In this case, there may be some obstruction to the flow of air and fluid out of the pleural space, causing air and fluid to collect and build up pressure. This prevents the remaining lung from reexpanding and can cause a mediastinal shift to the opposite side. The nurse’s first response is to assess the tubing for kinks or obstruction. Increasing the suction is not done without a health care provider’s prescription. The normal position of the drainage bottles is 2 to 3 feet (61 to 91.4 cm) below chest level. Clamping the tubes obstructs the flow of air and fluid out of the pleural space and should not be done.
Question 105.
The nurse is assessing a client who has a chest tube connected to a water seal chest tube drainage system. According to the illustration shown, what should the nurse do?
(a) Clamp the chest tube near the insertion site to prevent air from entering the pleural cavity.
(b) Notify the health care provider (HCP) of the amount of chest tube drainage.
(c) Add water to maintain the water seal.
(d) Lower the drainage system to maintain gravity flow.
Answer:
(d) Lower the drainage system to maintain gravity flow.
Explanation:
To promote chest tube drainage, the drainage system must be lower than the client’s lungs. The amount of drainage is not abnormal; it is not necessary to notify the HCP. The nurse should chart the amount and color of drainage every 4 to 8 hours. The chest tube does not need to be clamped; the tubing connection is intact. There is sufficient water to maintain a water seal.
Question 106.
The nurse is preparing to assist with the removal of a chest tube. Which dressing is appropriate at the site from which the chest tube is removed?
(a) adhesive strips
(b) petrolatum gauze
(c) dry 4x4 gauze
(d) no dressing is necessary
Answer:
(b) petrolatum gauze
Explanation:
Gauze saturated with petrolatum is placed over the site to make an airtight seal to prevent air leakage during the healing process. Dry dressings or adhesive strips are not used. An airtight dressing is needed until the insertion site is healed.
Question 107.
A nurse should interpret which finding as an early sign of a tension pneumothorax in a client with chest trauma?
(a) diminished bilateral breath sounds
(b) muffled heart sounds
(c) respiratory distress
(d) tracheal deviation
Answer:
(c) respiratory distress
Explanation:
Respiratory distress or arrest is a universal finding of a tension pneumothorax. Unilateral, diminished, or absent breath sounds is a common finding. Tracheal deviation is an inconsistent and late finding. Muffled heart sounds are suggestive of pericardial tamponade.
Question 108.
A nurse is to administer 10 mg of morphine sulfate to a client with three fractured ribs. The available concentration for this drug is 15 mg/mL. How many milliliters should the nurse administer? Round to one decimal point.
............................ mL.
Answer:
0.7 mL
10 mg :XmL= 15mg: 1 mL
15 mg × X mL = 10mg × 1 mL
15X = 10
X = 0.6667
X = 0.67mL
Question 109.
A young adult is admitted to the emergency department after an automobile accident. The client has severe pain in the right chest from contact with the steering wheel. What should the nurse do first?
(a) Reduce the client’s anxiety.
(b) Maintain adequate oxygenation.
(c) Decrease chest pain.
(d) Maintain adequate circulating volume.
Answer:
(b) Maintain adequate oxygenation.
Explanation:
Blunt chest trauma may lead to respiratory failure, and maintenance of adequate oxygenation is the priority for the client. Decreasing the client’s anxiety is related to maintaining effective respirations and oxygenation. Although pain is distressing to the client and can increase anxiety and decrease respiratory effectiveness, pain control is secondary to maintaining oxygenation. Maintaining adequate circulatory volume is also secondary to maintaining adequate oxygenation.
Question 110.
A client with rib fractures and a pneumothorax has a chest tube inserted that is connected to a water seal chest tube drainage system. The nurse notes that the fluid in the water seal column is fluctuating with each breath that the client takes. What is the significance of this fluctuation?
(a) An obstruction is present in the chest tube.
(b) The client is developing subcutaneous emphysema.
(c) The chest tube system is functioning properly.
(d) There is a leak in the chest tube system.
Answer:
(c) The chest tube system is functioning properly.
Explanation:
Fluctuation of fluid in the water seal column with respirations indicates that the system is functioning properly. If an obstruction were present in the chest tube, fluid fluctuation would be absent. Subcutaneous emphysema occurs when air pockets can be palpated beneath the client’s skin around the chest tube insertion site. A leak in the system is indicated when continuous bubbling occurs in the water seal column.
Question 111.
For a client with rib fractures and a pneumothorax, the health care provider prescribes morphine sulfate, 1 to 2 mg/h, given IV as needed for pain. The nursing care goal is to provide adequate pain control so that the client can breathe effectively. Which finding indicates the goal has been met?
(a) pain rating of 0 to 2 on a scale of 0 to 10 by the client
(b) decreased client anxiety
(c) respiratory rate of 26 breaths/min
(d) Pa02 of 70 mm Hg (9.31 kPa)
Answer:
(a) pain rating of 0 to 2 on a scale of 0 to 10 by the client
Explanation:
If the client reports no pain, then the objective of adequate pain relief has been met. Decreased anxiety is not related only to pain control; it could also be related to other factors. A respiratory rate of 26 breaths/min is not within normal limits, nor is the Pa02 of 70 mm Hg (9.31 kPa), but these values are not measures of pain relief.
Question 112.
A client undergoes surgery to repair lung injuries. Postoperative prescriptions include the transfusion of one unit of packed red blood cells at a rate of 60 mL/h. How long will this transfusion take to infuse?
(a) 2 hours
(b) 4 hours
(c) 6 hours
(d) 8 hours
Answer:
(b) 4 hours
Explanation:
One unit of packed red blood cells is about 250 mL. If the blood is delivered at a rate of 60 mL/h, it will take about 4 hours to infuse the entire unit. The transfusion of a single unit of packed red blood cells should not exceed 4 hours to prevent the growth of bacteria and minimize the risk of septicemia.
Question 113.
A client has been in an automobile accident, and the nurse is assessing the client for possible pneumothorax. What finding should the nurse immediately report to the health care provider?
(a) sudden, sharp chest pain
(b) wheezing breath sounds over affected side
(c) hemoptysis
(d) cyanosis
Answer:
(a) sudden, sharp chest pain
Explanation:
Pneumothorax signs and symptoms include sudden, sharp chest pain, tachypnea, and tachycardia. The nurse should report these to the health care provider (HCP). Other signs and symptoms include diminished or absent breath sounds over the affected lung, anxiety, and restlessness. Hemoptysis and cyanosis are not typically present with a pneumothorax.
Question 114.
The nurse is preparing the client diagnosed with pleural effusion for a left-sided thoracentesis. The X-ray shows fluid in the pleural cavity. During the preparation for the procedure, the client asks where the health care provider (HCP) will “put the needle.” Select the appropriate site from the diagram.
Answer:
The fluid typically localizes at the base of the thorax.
Question 115.
A client is undergoing a thoracentesis. What should the nurse monitor the client for during and immediately after the procedure? Select all that apply.
(a) pneumothorax
(b) subcutaneous emphysema
(c) tension pneumothorax
(d) pulmonary edema
(e) infection
Answer:
(a) pneumothorax
(b) subcutaneous emphysema
(c) tension pneumothorax
(d) pulmonary edema
Explanation:
(a), (b), (c), (d). Following a thoracentesis, the nurse should assess the client for possible complications of the procedure such as pneumothorax, tension pneumothorax, and subcutaneous emphysema, which can occur because of the needle entering the chest cavity. Pulmonary edema could occur if a large volume was aspirated causing a significant mediastinal shift. Although infection is a possible complication, signs of infection will not be evident immediately after the procedure.
Question 116.
When assessing a client with chest trauma, the nurse notes that the client is taking small breaths at first, then bigger breaths, and then a couple of small breaths, then 10 to 20 seconds of no breaths. How should the nurse record the breathing pattern?
(a) Cheyne-Stokes respiration
(b) hyperventilation
(c) obstructive sleep apnea
(d) Biot’s respiration
Answer:
(a) Cheyne-Stokes respiration
Explanation:
Cheyne -Stokes respiration is defined as a regular cycle that starts with normal breaths, which increase and then decrease followed by a period of apnea. It can be related to heart failure or a dysfunction of the respiratory center of the brain. Hyperventilation is associated with an increased rate and depth of respirations. Obstructive sleep apnea is recurring episodes of upper airway obstruction and reduced ventilation. Biot’s respiration, also known as “cluster breathing,” is periods of normal respirations followed by varying periods of apnea.
Question 117.
The nurse has placed the intubated client with acute respiratory distress syndrome (ARDS) in prone position for 30 minutes. Which factors would require the nurse to discontinue prone positioning and return the client to the supine position? Select all that apply.
(a) The family is coming in to visit.
(b) The client has increased secretions requiring frequent suctioning.
(c) The SpO2 and PO2 have decreased.
(d) The client is tachycardic with drop in blood pressure.
(e) The face has increased skin breakdown and edema.
Answer:
(c) The SPO2 and PO2 have decreased.
(d) The client is tachycardic with drop in blood pressure.
(e) The face has increased skin breakdown and edema.
Explanation:
(c), (d), (e). The prone position is used to improve oxygenation, ventilation, and perfusion. The importance of placing clients with ARDS in prone positioning should be explained to the family. The positioning allows for mobilization of secretions, and the nurse can provide suctioning. Clinical judgment must be used to determine the length of time in the prone position. If the client’s hemodynamic status, oxygenation, or skin is compromised, the client should be returned to the supine position for evaluation. Facial edema is expected with the prone position, but the skin breakdown is of concern.
Question 118.
To improve the oxygenation of a client with acute respiratory distress syndrome (ARDS) who is receiving mechanical ventilation, the nurse should place the client in which position?
(a) supine
(b) semi-Fowler’s
(c) lateral side
(d) prone
Answer:
(d) prone
Explanation:
Prone positioning is used to improve oxygenation in clients with ARDS who are receiving mechanical ventilation. The positioning allows for recruitment of collapsed alveolar units, improvement in ventilation, reduction in shunting, mobilization of secretions, and improvement in functional reserve capacity. When the client is supine, side- to-side repositioning should be done every 2 hours with the head of the bed elevated at least 30 degrees.
Question 119.
A client with acute respiratory distress syndrome (ARDS) has fine crackles at lung bases, and the respirations are shallow at a rate of 28 breaths/ min. The client is restless and anxious. In addition to monitoring the arterial blood gas results, what should the nurse do? Select all that apply.
(a) Monitor serum creatinine and blood urea nitrogen levels.
(b) Administer a sedative.
(c) Keep the head of the bed flat.
(d) Administer humidified oxygen.
(e) Auscultate the lungs.
Answer:
(a) Monitor serum creatinine and blood urea nitrogen levels.
(d) Administer humidified oxygen.
(e) Auscultate the lungs.
Explanation:
(a), (d), (e). ARDS may cause renal failure and superinfection, so the nurse should monitor urine output and urine chemistries. Treatment of hypoxemia can be complicated because changes in lung tissue leave less pulmonary tissue available for gas exchange, thereby causing inadequate perfusion. Humidified oxygen may be one means of promoting oxygenation.
The client has crackles in the lung bases, so the nurse should continue to assess breath sounds. Sedatives should be used with caution in clients with ARDS. The nurse should try other measures to relieve the client’s restlessness and anxiety. The head of the bed should be elevated to 30 degrees to promote chest expansion and prevent atelectasis.
Question 120.
The nurse is planning care for a client with a crushing chest injury. The client is in an intensive care unit, and the client’s vital signs have not stabilized. Which finding puts the client at risk for acute respiratory distress syndrome (ARDS)?
(a) history of smoking
(b) low serum potassium
(c) hypercapnia
(d) hypovolemia
Answer:
(d) hypovolemia
Explanation:
One of the major risk factors for development of ARDS is hypovolemic shock. Adequate fluid replacement is essential to minimize this risk. Smoking history does not directly a risk factor for ARDS. A low serum potassium level and hypercapnia are not risk factors for ARDS.
Question 121.
The nurse interprets which finding as an early sign of acute respiratory distress syndrome (ARDS) in a client at risk?
(a) elevated carbon dioxide level
(b) hypoxia not responsive to oxygen therapy
(c) metabolic acidosis
(d) severe, unexplained electrolyte imbalance
Answer:
(b) hypoxia not responsive to oxygen therapy
Explanation:
A hallmark of early ARDS is refractory hypoxemia. The client’s Pa02 level continues to fall, despite higher concentrations of administered oxygen. Elevated carbon dioxide and metabolic acidosis occur late in the disorder. Severe electrolyte imbalances are not indicators of ARDS.
Question 122.
A client with acute respiratory distress syndrome is showing signs of increased dyspnea. The nurse reviews a report of blood gas values (see report).
|
Blood Chemistry |
Result |
|
pH |
7.35 |
|
PaCO2 |
25 mm Hg (3.3 kPa) |
|
HCO3 |
22 mEq/L (22 mmoIfL) |
|
PO2 |
95 mm Hg (12.6 kPa) |
Which finding is abnormal?
(a) pH
(b) PaCO2
(c) HCO3
(d) PaO2
Answer:
(b) PaCO2
Explanation:
The normal range for PaCO2 is 35 to 45 mm Hg (4.7 to 6 kPa). Thus, this client’s PaCO2 level is low. The client is experiencing respiratory alkalosis (carbonic acid deficit) due to hyperventilation. The nurse should report this finding to the health care provider (HCP) because it requires intervention. The increase in ventilation decreases the PaCO2 level, which leads to decreased carbonic acid and alkalosis. The bicarbonate level is normal in uncompensated respiratory alkalosis along with the normal PaO2 level. Normal serum pH is 7.35 to 7.45; in uncompensated respiratory alkalosis, the serum pH is >7.45.
Question 123.
A client with acute respiratory distress syndrome is on a ventilator. The client’s peak inspiratory pressures and spontaneous respiratory rate are increasing, and the PO2 is not improving. Using the SBAR (Situation-Background-Assessment- Recommendation) technique for communication, the nurse calls the health care provider (HCP). What recommendation should the nurse give to the HCP?
(a) initiating IV sedation
(b) starting a high-protein diet
(c) providing pain medication
(d) increasing the ventilator rate
Answer:
(a) initiating IV sedation
Explanation:
The client may be fighting the ventilator breaths. Sedation is indicated to improve compliance with the ventilator in an attempt to lower peak inspiratory pressures. The workload of breathing does indicate the need for increased protein calories; however, this will not correct the respiratory problems with high pressures and respiratory rate. There is no indication that the client is experiencing pain. Increasing the rate on the ventilator is not indicated with the client’s increased spontaneous rate.
Question 124.
A client, diagnosed with acute pancreatitis 5 days ago, is experiencing respiratory distress. Which finding should the nurse report to the health care provider (HCP)?
(a) arterial oxygen level of 46 mm Hg (6.1 kPa)
(b) respirations of 12 breaths/min
(c) lack of adventitious lung sounds
(d) oxygen saturation of 96% on room air
Answer:
(a) arterial oxygen level of 46 mm Hg (6.1 kPa)
Explanation:
Manifestations of adult respiratory distress syndrome (ARDS) secondary to acute pancreatitis include respiratory distress, tachypnea, dyspnea, fever, dry cough, fine crackles heard throughout lung fields, possible confusion and agitation, and hypoxemia with arterial oxygen level below 50 mm Hg. The nurse should report the arterial oxygen level of 46 mm Hg (6.1 kPa) to the HCP. A respiratory rate of 12 is normal and not considered a sign of respiratory distress. Adventitious lung sounds, such as crackles, are typically found in clients with ARDS. Oxygen saturation of 96% is satisfactory and does not represent hypoxemia or low arterial oxygen saturation.
Question 125.
A client has the following arterial blood gas values: pH 7.52; PaO2 50 mm Hg (6.7 kPa); PaCO2 28 mm Hg (3.72 kPa); HCO2 -24 mEq/L (24 mmol/L). Based upon the client’s Pa02, which nursing clinical judgment should the nurse make?
(a) The client is severely hypoxic.
(b) The oxygen level is low but poses no risk for the client.
(c) The client’s Pa02 level is within normal range.
(d) The client requires oxygen therapy with very low oxygen concentrations.
Answer:
(a) The client is severely hypoxic.
Explanation:
Normal PaO2 level ranges from 80 to 100 mm Hg (10.7 to 13.3 kPa). When PaO2 falls to 50 mm Hg (6.7 kPa), the nurse should be alert for signs of hypoxia and impending respiratory failure. An oxygen level this low poses a severe risk for respiratory failure. The client will require oxygen-ation at a concentration that maintains the PaO2 at 55 to 60 mm Hg (7.3 to 8 kPa) or more.
Question 126.
To promote effective airway clearance in a client with acute respiratory distress, what should the nurse do?
(a) Administer oxygen every 2 hours.
(b) Turn the client every 4 hours.
(c) Administer sedatives to promote rest.
(d) Suction if cough is ineffective.
Answer:
(d) Suction if cough is ineffective.
Explanation:
The nurse should suction the client if the client is not able to cough up secretions and clear the airway. Administering oxygen will not promote airway clearance. The client should be turned every 2 hours to help move secretions; every 4 hours is not often enough. Administering sedatives to promote rest is contraindicated in acute respiratory distress because sedatives can depress respirations.
Question 127.
A nurse has received report on four clients. Which client would the nurse visit first?
(a) a client with congestive heart failure (CHF) who has gained 2 pounds overnight
(b) a client with tuberculosis who raised 50 mL of sanguineous sputum over the past 2 hours
(c) a client with C. difficile who continues to have loose, fouling smelling stools
(d) a client with chronic obstructive pulmonary disease (COPD) whose last report of oxygen saturation was 91%
Answer:
(b) a client with tuberculosis who raised 50 mL of sanguineous sputum over the past 2 hours
Explanation:
Sanguineous or bloody sputum (hemoptysis) is a sign of possible hemorrhage and may indicate vessel damage in the lungs; the nurse should assess this client first. The nurse should next evaluate the client with CHF and weight gain for additional signs of heart failure. Loose stools are expected for a client with C. difficile, and the nurse can delegate care to an unlicensed assistive personnel and follow up with this client later to determine the character and frequency of the stools. The client with COPD and an O2 saturation of 91% is within acceptable levels at this time, and the nurse can assess this client last.
Question 128.
A client with chronic obstructive pulmonary disease (COPD) has a signed living will with a do not resuscitate (DNR) request. While the wife was visiting the client, he had a cardiac arrest. The wife requested the client be resuscitated immediately. When the nurse hesitated to start resuscitation procedures, the wife threatened to sue the hospital. What should the nurse do? Select all that apply.
(a) Call the code for fear of being sued by the wife.
(b) Carry out the written DNR request and client wishes.
(c) Calmly remind the wife of the client’s wishes and DNR request.
(d) Notify the nurse manager of the situation.
(e) Call the chaplain to come and remain with the wife.
(f) Notify the health care provider (HCP).
Answer:
(b) Carry out the written DNR request and client wishes.
(c) Calmly remind the wife of the client’s wishes and DNR request.
(d) Notify the nurse manager of the situation.
(e) Call the chaplain to come and remain with the wife.
(f) Notify the health care provider (HCP).
Explanation:
(b), (c), (d), (e),(f). The nurse’s role is to carry out the client’s written wishes as indicated in the DNR and living will and the nurse should calmly remind the wife of the client’s wishes. The nurse next should notify the HCP who will determine that the client has died. The HCP also should reaffirm the client’s wishes with the wife. Chaplains are an important resource for families at times of loss.
They will remain with the families if they wish and attend to their needs. The nurse manager needs to be notified of the wife’s statement in order to notify risk management of a potential legal concern. Not carrying out the client’s written directions and wishes places the nurse and the facility under legal liability.
Question 129.
The nurse has received a change of shift report on clients. Which client should the nurse assess first?
(a) a client with COPD with a PaO2 of 56 mm Hg who is being discharged home on oxygen
(b) a client with asthma with respirations of 36 breaths/min whose wheezing has diminished
(c) a client with asthma who has a heart rate of 90 bpm and whose beta-blocker is scheduled to be administered now
(d) a client who is scheduled for an angiogram now and is ready to be transported
Answer:
(b) a client with asthma with respirations of 36 breaths/min whose wheezing has diminished
Explanation:
Respirations of 36 breaths/min and diminished wheezing are indicative of respiratory distress. This finding takes precedence over a client scheduled for an angiogram, a client with a heart rate if 90 bpm needing a scheduled beta-blocker,
or a client with a PaO2 of 56 mm Hg, which is indicated for a client being discharged home on oxygen.
Question 130.
The nurse is caring for a group of clients on a pulmonary unit. The nurse can delegate which task to unlicensed assistive personnel (UAP)?
(a) assisting a client with adjusting his or her nasal cannula
(b) making adjustments to flow rates based on client responses
(c) monitoring a client for adverse effects of oxygen therapy
(d) assessing a client for the best method of oxygen delivery
Answer:
(a) assisting a client with adjusting his or her nasal cannula
Explanation:
UAP can assist a client with the adjustment of his or her oxygen delivery device. Making adjustments based on client responses, monitoring for adverse effects, and assessing for the best methods of oxygen delivery are skills that require nursing judgments and can only be performed by a nurse.
Question 131.
A confused client with carbon monoxide poisoning experiences dizziness when ambulating to the bathroom. What should the nurse do?
(a) Put all four side rails up on the bed.
(b) Ask the unlicensed assistive personnel (UAP) to place restraints on the client’s upper extremities.
(c) Request that the client’s roommate put the call light on when the client is attempting to get out of bed.
(d) Check on the client at regular intervals to ascertain the need to use the bathroom.
Answer:
(d) Check on the client at regular intervals to ascertain the need to use the bathroom.
Explanation:
Confusion and vertigo are risk factors for falls. Measures must be taken to minimize the risk of injury. The nurse or UAP should check on the client regularly to determine needs regarding elimination. Restraints, including bed rails and extremity restraints, should be used only to ensure the person’s safety or the safety of others, and there must be a written prescription from a health care provider (HCP) before using them. The nurse should never ask the roommate of a client to be responsible for the client’s safety.
Question 132.
The nurse should use which type of precautions for a client being admitted to the hospital with suspected tuberculosis?
(a) standard precautions
(b) contact precautions
(c) droplet precautions
(d) airborne precautions
Answer:
(d) airborne precautions
Explanation:
Airborne precautions prevent transmission of infectious agents that remain infectious over long distances when suspended in the air (e.g., Mycobacterium tuberculosis, measles, varicella virus [chickenpox], and possibly SARS-CoV). The preferred placement is in an isolation single-client room that is equipped with special air handling and ventilation. A negative pressure room, or an area that exhausts room air directly outside or through HEPA filters, should be used if recirculation is unavoidable.
While standard precautions such as hand hygiene and wearing gloves and a gown is important, they are not sufficient to prevent transmission of tuberculosis. Contact precautions are used with clients with known or suspected infections who present an increased risk for contact transmission. Droplet precautions are intended to prevent transmission of pathogens spread through close respiratory or mucous membrane contact with respiratory secretions. Because these pathogens do not remain infectious over long distances in a health care facility, special air handling and ventilation are not required to prevent droplet transmission.
Question 133.
A client has developed a hospital-acquired pneumonia. When preparing to administer cephalexin 500 mg, the nurse notices that the pharmacy sent cefazolin. What should the nurse do? Select all that apply.
(a) Administer the cefazolin.
(b) Verify the medication prescription as written by the health care provider.
(c) Contact the pharmacy and speak to a pharmacist.
(d) Request that cephalexin be sent promptly.
(e) Return the cefazolin to the pharmacy.
Answer:
(b) Verify the medication prescription as written by the health care provider.
(c) Contact the pharmacy and speak to a pharmacist.
(d) Request that cephalexin be sent promptly.
(e) Return the cefazolin to the pharmacy.
Explanation:
(b), (c), (d), (e). One of the “five rights” of drug administration is “right medication.” Cefazolin was not the medication prescribed. The pharmacist is the professional resource and serves as a check to ensure that clients receive the right medication. Returning unwanted medications to the pharmacy will decrease the opportunity for a medication error by the nurse who follows the current nurse.
Question 134.
A nurse receives the taped change-of-shift report for assigned clients and prioritizes client rounds. In what order from first to last should the nurse assess these clients? All options must be used.
(a) a client who has an endotracheal tube and who will be transferred to a long-term respiratory care unit that day
(b) a client with type 2 diabetes who had a cerebrovascular accident 4 days ago
(c) a client with cellulitis of the left lower extremity with a fever of 100.8°F (38.2°C)
(d) a client receiving D5W IV at 125 mL/h with 75 mL remaining
Answer:
(a) a client who has an endotracheal tube and who will be transferred to a long-term respiratory care unit that day
(c) a client with cellulitis of the left lower extremity with a fever of 100.8°F (38.2°C)
(d) a client receiving D5W IV at 125 mL/h with 75 mL remaining
(b) a client with type 2 diabetes who had a cerebrovascular accident 4 days ago
Explanation:
(a), (c), (d), (b). Because two major complications of endotracheal tube intubation, inadvertent extubation and aspiration, can be catastrophic events, assessment of this client is the first priority. Cellulitis is a serious infection as there is inflammation of subcutaneous tissues; third spacing of fluid may promote the formation of a fluid volume deficit, which can be exacerbated by the fever due to insensible fluid loss. The nurse should assess this client next to determine current vital signs and fluid status.
The nurse should assess the client with the IV fluids next because the new bag of fluids will need to be hung in 30 to 40 minutes. IV therapy necessitates that the client be assessed for signs and symptoms of adequate hydration (moist mucous membranes, elastic skin turgor, vital signs within normal limits, adequate urine output, and level of consciousness within normal limits), and the IV access site needs to be assessed. From the information provided, there is no indication that the client who had the cerebrovascular accident is unstable. Thus, this client is the last priority for assessment.
Question 135.
The nurse is a member of a team that is planning a client-centered, community-based approach to care of clients with chronic obstructive pulmonary disease. In which areas should the team focus on improving quality of care and delivery? Select all that apply.
(a) the community
(b) clinical information systems
(c) delivery system design
(d) administrative leadership
(e) acute care setting
Answer:
(a) the community
(b) clinical information systems
(c) delivery system design
Explanation:
(a), (b), (c). The process of changing a health care system from an acute care model to a community- based care model uses continuous quality improvement methods. The goal is to improve the health of chronically ill clients. Areas for improvement include health systems, delivery system design, decision support, clinical information systems, self-management support, and the community. This system requires health care services that are client centered and coordinated among members of the health care team and the client and the family. These changes do not focus on the administrative leadership or the care in the acute care setting alone.
Question 136.
The nurse is caring for a client admitted for pneumonia with a history of hypertension and heart failure. The client has reported at least one fall in the last 3 months. The client may ambulate with assistance, has a saline lock in place, and has demonstrated appropriate use of the call light to request assistance. Using the Morse Fall Scale (see chart), what is this client’s total score and risk level?
|
Item |
Scale |
Scoring |
|
1. History of falling; immediate or within 3 months |
No 0 |
|
|
2. Secondary diagnosis |
No 0 |
|
|
3. Ambulatory aid Bed rest/nurse assist Crutch es/ca ne/wa I ke r |
0 |
|
|
4. IV/Heparin Lock |
No 0 |
|
|
5. Gait/Transferring Normal/bedrest/ immobileWeak Impaired |
0 |
|
|
6. Mental status Oriented to own ability Forgets limitations |
0 |
|
(a) 20, low risk
(b) 30, medium risk
(c) 40, medium risk
(d) 60, high risk
Answer:
(d) 60, high risk
Explanation:
Several factors designate this client as a high fall risk based on the Morse Fall Scale: history of falling (25), secondary diagnosis (15), plus IV access (20). The client’s total score is 60. There is also concern that the client’s gait is at least weak if not impaired due to hospitalization for pneumonia, which may add to the client’s fall risk. After evaluating the client’s risk, the nurse must develop a plan and take action to maximize the client’s safety.
Question 137.
The nurse is caring for a client who has been placed on droplet precautions. Which protective gear is required to take care of this client? Select all that apply.
(a) gloves
(b) gown
(c) surgical mask
(d) glasses
(e) respirator
Answer:
(a) gloves
(b) gown
(c) surgical mask
(d) glasses
Explanation:
(a), (b), (c), (d). Gloves, gown, surgical mask, and eye protection/glasses are worn to protect health care workers and to help prevent the spread of infection when clients are placed in droplet isolation. Because droplets are too heavy to be airborne, a respirator is not required when caring for a client in droplet precautions.
Question 138.
While making rounds, the nurse finds a client with chronic obstructive pulmonary disease sitting in a wheelchair, slumped over a lunch tray. After determining the client is unresponsive and calling for help, what should the nurse do next?
(a) Push the “code blue” (emergency response) button.
(b) Call the rapid response team.
(c) Open the client’s airway.
(d) Call for a defibrillator.
Answer:
(c) Open the client’s airway.
Explanation:
The nurse has already called for help and established unresponsiveness, so the first action is to open the client’s airway; opening the airway may result in spontaneous breathing and will help the nurse determine whether or not further intervention is required. Pushing the “code blue” button may not be the appropriate action if the client is breathing and becomes responsive once the airway is open. A quick assessment upon opening the client’s airway will help the nurse to determine if the rapid response team is needed. Calling for a defibrillator may not be the necessary or appropriate action once the client’s airway has been opened.
Question 139.
The nurse is caring for a client with pneumonia who is confused about time and place and has intravenous fluids infusing. Despite the nurse’s attempt to reorient the client and then provide distraction, the client has begun to pull at the IV tubing. After increasing the frequency of observation, in which order should the nurse implement interventions to ensure the client’s safety? All options must be used.
(a) Review the client’s medications for interactions that may cause or increase confusion.
(b) Assess the client’s respiratory status including oxygen saturation.
(c) Ensure the client does not need toileting or pain medications.
(d) Contact the health care provider and request a prescription for soft wrist restraints.
Answer:
(b) Assess the client’s respiratory status including oxygen saturation.
(c) Ensure the client does not need toileting or pain medications.
(d) Contact the health care provider and request a prescription for soft wrist restraints.
(a) Review the client’s medications for interactions that may cause or increase confusion.
Explanation:
(b), (c), (d), (a). The nurse should first assess the client’s respiratory status to determine if there is a physiological reason for the client’s confusion. Other physiological factors to assess include pain and elimination. Safety needs including medication interactions should then be evaluated. Requesting restraints in order to maintain client safety should be used as a last resort.
Question 140.
The nurse’s assignment consists of four clients. After receiving shift report, in which order from first to last should the nurse assess these clients? All options must be used.
(a) an 85-year-old client with bacterial pneumonia, temperature of 102.2°F (42°C), and short ness of breath
(b) a 60-year-old client with chest tubes who is 2 days postoperative following a thoracotomy for lung cancer and is requesting something for pain
(c) a 35-year-old client with suspected tuberculosis who has a cough
(d) a 56-year-old client with emphysema who has a scheduled dose of a bronchodilator due to be administered, with no report of acute respiratory distress
Answer:
(a) an 85-year-old client with bacterial pneumonia, temperature of 102.2°F (42°C), and shortness of breath
(b) a 60-year-old client with chest tubes who is 2 days postoperative following a thoracotomy for lung cancer and is requesting something for pain
(d) a 56-year-old client with emphysema who has a scheduled dose of a bronchodilator due to be administered, with no report of acute respiratory distress
(c) a 35-year-old client with suspected tuberculosis who has a cough
Explanation:
(a), (b), (d), (c). The elderly client with pneumonia, an elevated temperature, and shortness of breath is the most acutely ill client described and should be the client with the highest priority. The elevated temperature and the shortness of breath can lead to a decrease in the client’s oxygen levels and can predispose the client to dehydration and confusion. Then the nurse should assess the client with the thoracotomy who is requesting pain medication and administer any needed medication. The client with emphysema should be the next priority so that the bronchodilator can be administered on schedule as close as possible. The nurse would then assess the client with suspected tuberculosis and a cough.
Question 141.
The unlicensed assistive personnel (UAP) reports to the registered nurse that a client admitted with pneumonia is very diaphoretic. The nurse reviews the vital signs in the medical record obtained by the UAR What should the nurse do? Select all that apply.
|
Time |
0800 |
1000 |
1200 |
|
Temperature |
38.3°C |
|
38.8°C |
|
Pulse |
90 |
104 |
118 |
|
Respirations |
16 |
18 |
24 |
|
Blood Pressure |
112/74 |
110/68 |
116/78 |
|
Spo2 |
93% |
92% |
92% |
(a) Assure the client is maintaining complete bed rest.
(b) Check the urine output.
(c) Ask the client to drink more fluids.
(d) Notify the health care provider.
(e) Administer acetaminophen as prescribed.
Answer:
(b) Check the urine output.
(c) Ask the client to drink more fluids.
(e) Administer acetaminophen as prescribed.
Explanation:
(b), (c), (e). A client with pneumonia experiencing diaphoresis is at risk for dehydration and increased temperature and heart rate. The fluid status, intake, and urine output should be monitored closely. The client is febrile, causing an increase in heart rate. Fluid volume deficit may also increase the heart rate. The underlying cause of the tachycardia can be treated with acetaminophen and increased intake of fluids. Bed rest limits lung expansion, and sitting up and deep breathing should be encouraged in a client with pneumonia. The blood pressure is stable enough to allow the client to get out of bed to the chair, with assistance to ensure safety. It is not necessary to notify the HCP.